Article: J. Backus (Germany)
Overland Casualty Evacuation - a Component of the Evacuation Chain
One of the paramount objectives of the medical support of personnel in the field is the provision of mobile medical first aid and subsequent evacuation of casualties in appropriately designed casualty transport vehicles or under the supervision of mobile physician teams (BAT: Bewegliche Arzttrupps) or paramedic teams (SanTrp: Sanitätstrupps).
This article provides an overview and discusses the future of armoured overland casualty transport vehicles employed by the Joint Medical Services of the Bundeswehr (ZSanDstBw: Zentraler Sanitätsdienst der Bundeswehr).
Basic concepts
The ZSanDstBw of the German Bundeswehr has developed a military heath strategy that is sustainable, is adapted to the needs of combat and conforms to current medical and technological standards. This is based on a medical support concept designed to meet the specific requirements of the armed forces which guarantees that personnel will receive treatment with a quality of outcome equivalent to that which would be expected were they to undergo treatment in the homeland.
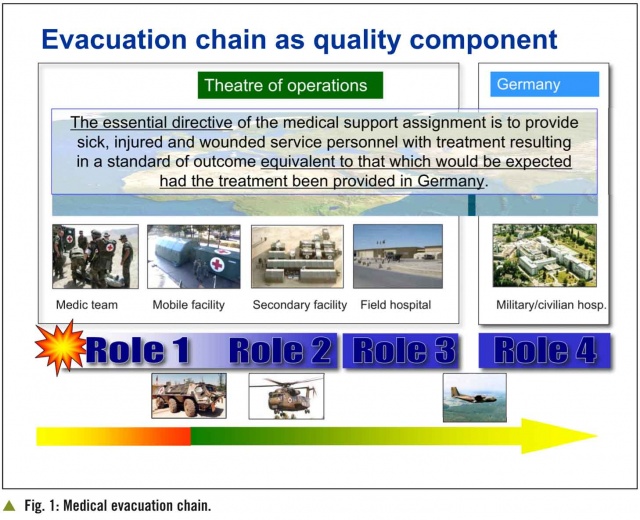
Early, direct and specialised medical intervention, particularly in the sector of emergency medicine, is essential to ensure the survival of casualties and the standard of outcome for sick, injured and wounded personnel. If lives are to be saved and subsequent complications prevented, treatment must be commenced at a point as close as possible to that at which the wound/injury was sustained and supplemented by appropriate follow-up treatment. This is provided through the evacuation chain system, which is designed to meet the specific needs of the various theatres of operations. The individual components are:
n On-site self-help and 'buddy-buddy' support.
n First aid and emergency medical measures (NATO Role 1).
n Initial emergency surgical intervention (NATO Role 2).
n Specialist acute treatment in the theatre of operations (NATO Role 3).
n Subsequent hospitalisation/out-patient treatment and rehabilitation in Germany (NATO Role 4).
Within its specific components, the evacuation chain provides for flexible casualty management. Casualties are transported directly to the medical facility that can provide them with the most suitable level of treatment.
The organisation of casualty transport is an integral element of the evacuation chain and thus of the emergency medical support concept. The objective is to bring casualties, following stabilisation of their status, as rapidly and in as non-incapacitating a form as possible to the nearest medical facility. In the field, the underlying requirement is to ensure that appropriate medical treatment can be provided at all times and all locations of the combat zone and that medical supervision is provided en route during secondary transport to another medical facility (the “continuum of care”).
The German System Capability Requirement (SFF) “Transport of armed forces casualties” (20 June 2005) defines casualty transport as “the targeted and appropriate evacuation of wounded, injured and sick personnel in accordance with military and medical requirements. The vehicles to be used for transport are to be identified using the international Red Cross symbol (red cross on white background), with the exception of such vehicles that are only temporarily medically equipped for this purpose.”
Of course, speed is one of the major determining factors when it comes to casualty evacuation. The requirements for specialised casualty transport conform to the German domestic emergency and disaster medicine specifications. There are different forms of casualty transport: airborne (AIRMEDEVAC ) and ground-based (GROUNDMEDEVAC) evacuation. In both cases, the aim is to evacuate casualties, without the necessity for frequent change of specialised transport vehicle, to a suitable medical facility with the necessary capacity as rapidly as possible. At the same time, specialist medical monitoring and treatment of the casualties must be provided en route over the whole of the journey.
In view of experience obtained during exercises and in the field and theoretical considerations, it is apparent that if NATO medical services are to provide qualitatively adequate medical support, they must be provided with land-based casualty transport vehicles that are, among other things, highly mobile and appropriate to the environment of the particular combat zone. Hence, a casualty transport vehicle must conform to the following operational requirements:
➤ It must be designed so that in all combat situations – even in extreme climatic conditions and/or on difficult terrain – casualties can be evacuated in such a way that there is maximum mitigation of their condition.
➤ It must be equipped so that casualties can be monitored and treated en route during the entire journey.
➤ It must be provided with the maximum extent of protection for casualties, medical personnel and equipment that is consistent with the vehicle’s design and the level of potential threat.
➤ It must be such that it can provide for the delivery and transfer of casualties as appropriate to the nature and severity of their wounds/injuries and the military situation. It must also be possible to track the movement and status of patients during the journey.
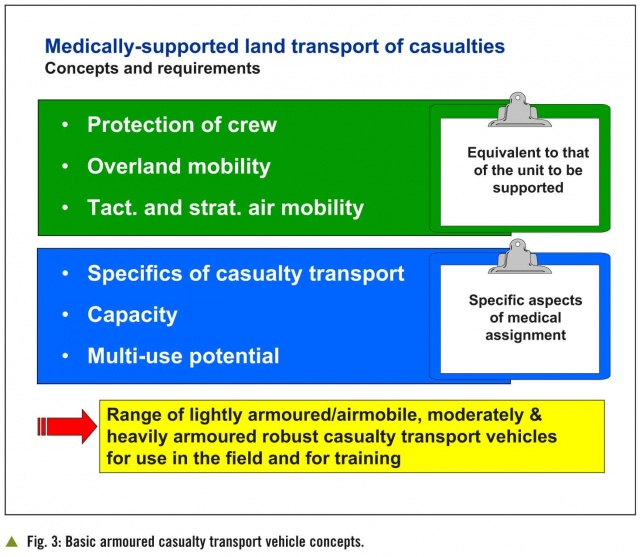
In order to meet the stipulations of the System Capability Requirement “Transport of armed forces casualties”, particularly in view of the changing conditions on the battlefield, the Medical Services of the Bundeswehr now have a need for suitably armoured transport vehicles that provide the same level of protection, have the same mobility and wherever possible, the same constructional profile as those of the unit to be supported. In addition to general maintenance support, the Medical Services also need to be able to decisively and flexibly act during operations involving heavy combat against a militarily organised enemy and against adversaries that use asymmetrical tactics.
The potential deployment situations and the different forms of army and other land-based force units requiring support mean that the Medical Services need to have a certain range of various casualty evacuation vehicles at their disposal. Here, the desideratum is also to use the same vehicle platforms as the force being supported and to equip these with a tailored command information / command and operation system which will allow these to be managed through a future integrated operational command set-up. Casualty evacuation vehicles need to be made available for transport by land, sea and air that meet the medical requirements of all feasible battlefield scenarios.
Basic designs and types of armoured, land-based
casualty evacuation vehicles
The capacity for armoured, land-based evacuation of casualties is of essential importance if the viability of any form of combat force is to be maintained. To reiterate the maxim outlined above: medical support services must thus be provided with vehicles that offer the same level of mobility and protection as those employed by the units to be supported!
The underlying need is thus for “lightly armoured, moderately heavily armoured and heavily armoured medical transport vehicles”. The vehicle versions currently available differ mainly in terms of the number of casualties they are able to accommodate and their operational potentials (Fig. 3).
Lightly armoured medical transport vehicle (lgSanKfz)
Vehicles that can be brought to the theatre of operations using the CH53 transport helicopter are required for the medical support of missions involving airmobile units. The extent of protection, mobility and medical equipment that can be provided in such vehicles is thus restricted by the maximum payload that can be carried and the hold capacity/ dimensions of the aircraft. The current airmobile physician unit (LBAT: Luftbeweglicher Arzttrupp) concept involves an emergency physician vehicle and a casualty evacuation vehicle based on the WOLF HGV chassis, with a long wheel base and modular shrapnel protection (MSS). These have since reached the limits of their technical and operational capacity and, because two vehicles are used, two crews are also necessary. It is now planned to replace these with a single vehicle concept in the form of an “armoured airmobile medical transport vehicle”. Unfortunately, the proposed solutions to date for a vehicle in this form would exceed maximum permitted load capacities. The armament industry thus here needs to harness all its innovation potential to develop a vehicle that would meet all given specifications.
However, there is already a need for small, highly mobile and armoured vehicles that are capable of negotiating the mainly very constricted and often mountainous tracks and terrain in the zones in which the German contingent is operating in the north of Afghanistan. Although the present LBAT-WOLF vehicles are sufficiently manoeuvrable, they cannot be considered as a long-term solution because of their lack of armour. For this reason, a medical version of the EAGLE IV vehicle, already adopted by the land forces, has been developed and has been deployed in Afghanistan under the name EAGLE IV BAT since 2011.
(1)Specifications for a lightly armoured medical transport vehicle (lgSanKfz)
n Medically equipped for the transport of one intensive care stretcher case.
n Crew: Three man team.
n Clearance above stretcher approx. 60 cm or, assuming this is not possible, optimumergonomic adaptation within the given parameters.
n “Universal casualty transport” design
(2)Mobility and protection
n Should conform to requirements with regard to mobility and deployability and offer a level of protection equivalent to that provided to the unit being supported.
Moderately heavily armoured medical transport vehicle (mgSanKfz)
Because of the cross-functional assignment profile of the Bundeswehr, the moderately heavily armoured medical transport vehicle will continue to represent the backbone of the armoured casualty evacuation fleet used by the Joint Medical Services. This is used for medically-supported primary transport of casualties, injured and sick personnel, irrespective of severity of status, from the site at which the injury/wound was sustained to a Role 1 or 2 medical facility. The patients are constantly monitored and their vital signs secured, while the armour provides protection to those within the vehicle.
Because of the need for rapid first aid on-site and for treatment and prophylaxis of any life-threatening complications that develop during evacuation or transport, the moderately heavily armoured medical transport vehicle must be fitted with the necessary medical equipment.
However, the YAK HGV in its BAT version that is currently being used in this role has an insufficient retrofit capacity, meaning that it will not continue to be used as the standard moderately heavily armoured medical transport vehicle in future.
A new moderately heavily armoured medical transport vehicle needs to be developed that, in terms of mobility and medical capabilities, will fit happily between the two extremes of the lightly armoured and heavily armoured casualty transport vehicles. Necessary transport requirements mean that this vehicle will need to accommodate two stretcher cases.
(1)Specifications for a moderately heavily armoured medical transport vehicle (mgSanKfz)
n Medically equipped for the transport of at least two stretcher cases (to include one intensive care case).
n Crew: up to four.
n The ergonomic design of the interior (working height) must be such that the medical personnel can adequately attend to the casualties.
n Clearance above stretchers approx. 60 cm in each case or, assuming this is not possible, optimum ergonomic adaptation within the given parameters.
n “Universal casualty transport” design
(2)Mobility and protection
n Should conform to requirements with regard to mobility and offer a level of protection equivalent to that provided to the unit being supported.
n Maximum weight relative to that of the lightly armoured and heavily armoured medical transport vehicles.
Heavily armoured medical transport vehicle (sgSanKfz)
Armoured combat units must also be supported in all deployment situations by casualty evacuation units that have an equivalent level of protection and can continue to shadow the combat unit irrespective of the battlefield terrain. The heavily armoured GTK BOXER medical transport vehicle has been developed as the successor to the armoured ambulance (KrKwPz) M 113. It is designed to be used for the support of armoured combat units and other units that employ vehicles derived from the GTK BOXER concept.
(1)Specifications for a heavily armoured medical transport vehicle (sgSanKfz)
n Medically equipped for the transport of at least three stretcher cases (to include oneintensive care case).
n Crew: up to four.
n The ergonomic design of the interior (working height) must be such that the medical personnel can adequately attend to the casualties.
n Clearance above stretchers approx. 60 cm in each case or, assuming this is not possible, optimum ergonomic adaptation within the given parameters.
n “Universal casualty transport” design
(2)Mobility and protection
n Should conform to requirements with regard to mobility and offer a level of protection equivalent to that provided to the unit being supported.
Medical capabilities
In the case of the medical vehicles used to date, their equipment determined whether they were used by a mobile physician team or a paramedic team. This meant that the individual vehicles were essentially permanently assigned to their role as either a mobile physician or paramedic team vehicle and could not be reassigned for use for the other purpose.
To enhance flexibility in the field, this concept is to be abandoned in favour of a so-called “universal casualty transport” design as in Fig. 4.
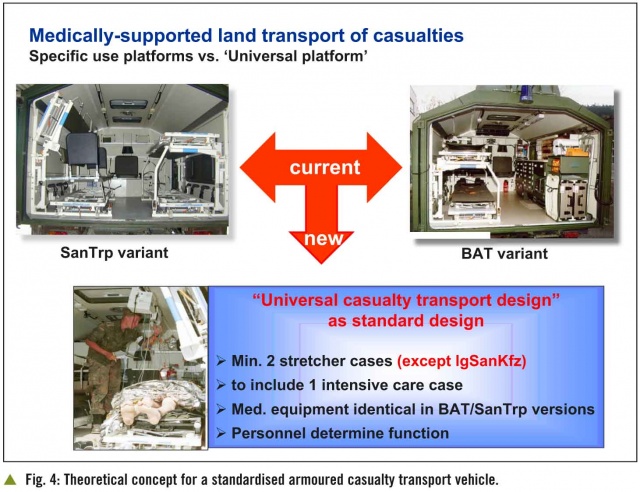
This design will provide the equipment required by a mobile physician team (BAT). This means that the differentiation between vehicles as “BAT” and “SanTrp” will no longer be based on material considerations but solely on the nature of the personnel manning them (a “BAT” team includes a medical officer, the “SanTrp” consists of paramedics only).
Other vehicle versions
TPz FUCHS San
With the commencement of the Bundeswehr’s participation in KFOR in 1999, armoured transport vehicles (TPz) used by land forces were rapidly adapted to medical transport vehicles to plug the perceived gap when it came to casualty transport in the field.
The ZSanDstBw now uses the TPz FUCHS San in a range of different versions to support the German contingents of KFOR and ISAF and at home for training purposes. All vehicles currently in use in Afghanistan are being reequipped with modular armour systems, IED/mine protection and BAT medical equipment.
The effectiveness of the protective and medical capacities of the TPz FUCHS have been demonstrated under combat conditions, and this vehicle will continue to be employed until a sufficient number of alternative heavily and moderately heavily armoured medical transport vehicles become available.
However, it must be pointed out that its dimensions and weight mean that the tactical mobility of the vehicle is limited in built-up areas and when it comes to accompanying patrols on narrow roadways and tracks. In addition, it can provide medically-supported transport for one casualty only.
Armoured casualty transport container (GVTC)
In order to ensure that the patient admission capacities of primary medical facilities are not overwhelmed during missions involving high levels of threat and combat, it is necessary to be able to provide protection to casualties whose status has been stabilised while these are transferred to other facilities for further treatment (secondary transport). A container-based system has been designed for this purpose that provides protection against mines, missiles and also lateral protection against IEDs. The GVTC can accommodate four stretcher cases and six seated casualties or six moderately severely wounded stretcher cases. The containers are designed to be mounted on the MULTI FSA HGV chassis.
BV 206 S
To recapitulate, it is necessary that casualty transport vehicles are provided with the same level of protection and mobility as the vehicles employed by the unit requiring medical support.
The vehicles used by the elements of the ZSanDstBw assigned to support operations undertaken by the Gebirgsjäger (mountain infantry) units of the Bundeswehr must thus conform to the specialised multi-terrain vehicles used by these troops.
Used to date for this purpose was the BV 206 S in both SanTrp and BAT variants. This vehicle has the necessary mobility thanks to its four-tracked drive, but has already reached the limits of its medical capabilities in terms of performance and retrofit capacity. A new suitable successor vehicle thus needs to be found that meets the requirements in terms of mobility and medical needs.
Summary
It is only right and proper that serving personnel who are sick, injured or wounded should expect that the medical support provided to them in the field will result in a standard of outcome equivalent to that which they would expect were they to receive treatment in the homeland. This is a fundamental humanitarian objective and the awareness of this has a positive effect on the motivation and morale of troops. It is thus also necessary to provide for medically-supported, protected casualty transport if this aspiration is to be met, particularly in theatres of combat.
Employing a concept involving three basic types of vehicle – lightly armoured, moderately heavily armoured and heavily armoured medical transport vehicles – the Medical Services are able to meet the requirements of their highly complex medical assignments on missions throughout the world. They are able to provide a tactically suitable casualty transport vehicle to support combat units operating in all types of environments. The other vehicle variants available to the Medical Services represent useful additions to the range of armoured casualty transport vehicles that can be employed in the field.
References: ref@mci-forum.com
Date: 12/19/2012
Source: MCIF 4/13