Report: H.-U. HOLTHERM (GERMANY)
Development of a multinational Deployment Health Surveillance Capability (DHSC) for NATO
At the 2002 NATO Summit still under the impression of the terror attacks in the United States, decisive capability gaps were
shown to exist within NATO. Among other issues, warnings were raised about the lack in capability for the near-real-time (NRT)
detection of disease outbreaks and the determination of whether these outbreaks are to be attributed to the use of biological
weaponry or to natural causes. Since 2003, under the lead of NATO Allied Command Transformation (ACT), existing capabilities
and systems of NATO partners have therefore been identified and examined as to their suitability for operational use in NATO
deployments.
Introduction
Even during high intensity military conflicts, like in Afghanistan and Iraq, infectious diseases still represent a major cause for hospitalization and loss of soldier’s duty days in the deployment areas.
Soldiers duty days lost during past military conflicts due to:
Battle injuries: 5 – 25 %
Non battle injuries: 5 – 10 %
Infectious diseases: 65 – 80 %
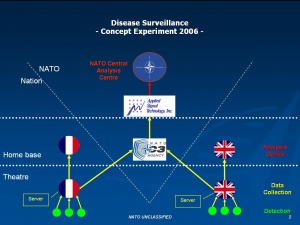 Architecture of the 2006 experiment
Architecture of the 2006 experiment
Therefore the control and minimization of infectious diseases among deployed soldiers is of highest operational importance for the military medical services of the participating nations.
Especially in deployment areas with low hygienic standards like in certain African and South- or Central Asian areas, infection control can be an essential factor in order to sustain operational readiness of the deployed troops.
A second factor, especially in asymmetric warfare and counterinsurgency operations, is that bioterrorist threats always have to be considered as to their possibly high impact on the operational readiness of deployed troops.
Due these two important operational facts, Military Medical Services of NATO have to provide not only state-of-the-art emergency medicine- and curative medicine assets but - equally important - mission tailored preventive medicine- and public health assets in order to guarantee a high level of Force Health Protection (FHP) for the deployed soldiers.
An important part of Force Health Protection and especially for the control of infectious diseases is the provision of efficient disease surveillance systems and -capabilities for a timely and standardized detection of infectious disease outbreaks and epidemics. The DHSC uses the following modified versions of definitions for Disease Surveillance and - more specific - Near-Real-Time (NRT) Syndromic Surveillance:
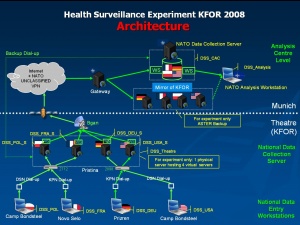 Architecture of the 2008 experiment
Disease Surveillance is:
Architecture of the 2008 experiment
Disease Surveillance is:
The ongoing and systematic collection and analysis of data and the provision of information which leads to action being taken to prevent and control a disease (naturally occurring or deliberately caused)
NRT Syndromic Surveillance is:
Early detection of- and action against deliberately caused or natural outbreaks of disease through the statistical analysis of defined signs and symptoms of disease
In order to provide an efficient disease surveillance capability, a combination of different parts of subject matter- and technical expertise is needed.
At first, high level epidemiological expertise is essential for quality health data collection and analysis as well as for the production of the consequent recommendations.
Secondly, high level Information Technology (IT) -expertise is needed for the development and programming of useful, efficient and operational disease surveillance software and for the determination of suitable IT hardware.
Thirdly, the specific aspects of military mission related necessities like classification issues, confidentiality and - when dealing with NATO missions - multinationality have to be considered. This makes operational and military expertise a conditio sine qua non for a military disease surveillance capability.
Finally, state-of-the-art IT-hardware systems and mission tailored software solutions are needed to ensure safe and stable data collection, storage, transmission and automated analysis.
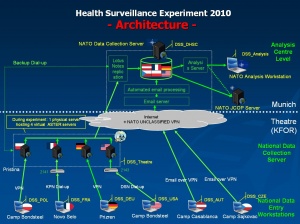 Architecture of the 2010 experiment
Architecture of the 2010 experiment
Furthermore it has to be considered that a comprehensive and integrated Military Disease surveillance capability should integrate different and multidisciplinary surveillance aspects like laboratory surveillance, veterinary surveillance, entomological surveillance and standardized coded surveillance, like the International Classification of Diseases (ICD 10).
The periodicity of disease surveillance reporting can range from Near-Real-Time syndromic-surveillance as an early warning tool up to routine reporting periods e.g. weekly or monthly for laboratory- or ICD 10 coded surveillance.
An absolute necessity for a NATO DHSC is interoperability, multinationality and accessibility. This is based on the fact that NATO has 28 member states and nearly all NATO missions are multinational. In the International Security Assistance Force (ISAF) mission in Afghanistan even non NATO members are participating and therefore should be included in the deployment health surveillance effort.
History of the DHSC development for NATO:
- Identification of the Disesase Suveillance Capability gap in NATO:
During the 2002 Prague NATO Summit of Heads of State and Government - still in the light of the terrorist attacks in the United States in 2001 – decisive capability gaps in NATO’s abilities to react to asymmetric threats were identified. Among these capability gaps was the lack of an early warning disease surveillance system to detect naturally occurring or deliberately caused outbreaks of infectious disease. The NATO Summit tasked the Chemical, Biological, Radiation and Nuclear (CBRN) Defense - and the Medical communities within NATO to identify existing systems within the armed forces of its member states. NATO Allied Command Transformation (NATO ACT) in Norfolk, USA was determined to be the lead command for this task.
Until 2005 several national NRT surveillance capabilities had been identified and tested, concerning their ability to serve NATO’s requirements. Finally two syndromic surveillance systems were identified, which could possibly close the early warning gap: the British (GBR) Portable Remote Illness and Symptoms Monitor (PRISM) system and the French (FRA) system “Alert et Surveillance en temps Reel” (ASTER).
- Multinational NRT Surveillance System experiment series 2006 - 2010:
In 2006, an ACT led table-top experiment tested the FRA and GBR systems and concepts of syndromic surveillance against the concept of an integrated and multinational NRT surveillance capability. For this table-top experiment 2 disease outbreak scenarios (deliberately caused pulmonary anthrax and a naturally occurring shigellosis outbreak) within a multinational NATO Coalition Force deployed to Afghanistan were developed by epidemiologists. The datasets of these disease outbreak scenarios were fed into the respective NRT surveillance systems. The NATO Consultation, Command and Control Agency (NC3A) provided the necessary IT support for the experiment’s IT infrastructure and network.
The results of this initial experiment should influence the decision about the most suitable early warning system and -concept for NATO. The Bundeswehr Medical Office in Munich was chosen to be the Central Analysis- and Evaluation Center for this experiment due to its proven capabilities in the field of Public Health and Medical Intelligence as well as its Medical CBRN Defense- and Veterinary Medicine components.
The results of the 2006 table-top experiment clearly showed:
- The integrated and multinational NRT disease surveillance concept showed better sensitivity (earlier detection) compared with the respective national (FRA / GBR) concepts.
- The integrated and multinational NRT disease surveillance concept showed better specificity (better ability to detect the real cause of disease) compared with the respective national (FRA / GBR) concepts.
- The necessity of a core team of subject matter experts (epidemiologists, IT-specialists and experienced military personnel) in order to run the central analysis center.
- The suitability of the Bundeswehr Medical Office to serve as the home institution of a DHSC for NATO
Considering the positive results of the 2006 table-top experiment, NATO ACT decided to proceed with the DHSC experimentation in a real NATO deployment area as a life experiment. The Kosovo Force (KFOR) was chosen as the most appropriate NATO mission, where this experiment could be conducted. After intensive preparatory work, this second experiment was performed in 2008 in the KFOR theatre. Actively participating nations were Germany, France, USA and Poland with their military contingents in Kosovo.
NC3A was coordinating and supporting in all IT aspects of the experiment. From this experiment onwards, the French NRT surveillance system ASTER was used as the IT-platform, because it had proven its suitability for operational use and was available without cost for the NATO experiments. The British PRISM system had been commercialized and was no longer available for experimental use.
The focus of this experiment was to test the technical suitability of the multinational NRT surveillance concept to be operated in a real NATO mission. Surveillance data collection was done by medical doctors on a disease symptom level in the Role 1 units of the participating nations. The collected data were transmitted from the Role 1 units to a theatre server in KFOR Headquaters (HQ) in Pristina. After anonymization, these data were sent via satellite to the analysis server in the Central Analysis Center in Munich.
A multinational team comprised of subject matter experts of the participating nations received and analyzed the data before they provided the resulting feed back to KFOR HQ.
In a third DHSC experiment again in KFOR in 2010, different software applications and data transmission modes were tested (internet vs satellite); the number of participating nations was enhanced, so that besides Germany, France, USA and Poland, at this experiment Austria and the Czech Republic were actively participating as well. Additionally a social science evaluation of the human factor influences in the Central Analysis Center in Munich was conducted by French scientists.
Results of the 2008 and 2010 KFOR experiments were:
- Multinational NRT syndromic surveillance for a military mission abroad is technically feasible
- NRT surveillance training for the data entry personnel (Role 1 physicians) using the ASTER system can be done in short courses (1/2 day)
- Compliance of the data entry personnel was very good.
- Besides NRT syndromic surveillance as an early warning tool, a routine periodic surveillance tool has to be integrated into the DHSC in order to achieve situational awareness concerning the health status of deployed forces
- Further testing and experimentation is necessary in order to stabilize and professionalize the NRT surveillance system for multinational use
- The EpiNATO routine disease reporting and surveillance tool of NATO is unsatisfactory for operational use and has to be improved
NATO ACT, NATO Allied Command Operations (ACO) and the participating nations evaluated the results of the NRT surveillance experiments as a successful step on the way to close the identified surveillance capability gap.
Considering the successful performance of the 2006 -2010 NRT Surveillance experiment series, the Committee of the Chiefs of Military Medical Services in NATO (COMEDS), which is representing the Surgeons General of all NATO nations, supported the implementation of a Deployment Health Surveillance Capability (DHSC) for NATO in Munich.
Implementation of the DHSC in Munich:
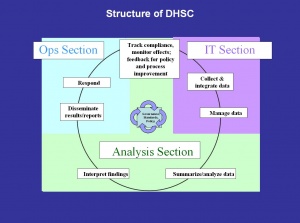
In 2010, the German Bundeswehr Joint Medical Service provided the infrastructure and framework for a multinational DHSC in Munich, by implementing a DHSC branch within the Department of Preventive Medicine in the Bundeswehr Medical Office. The structure of this DHSC branch includes an Analysis Section, an IT-Section and an Operations Section.
Germany filled the positions of the branch head and of 2 Non Commissioned Officers (NCO) in the IT- and Operations section in mid 2010. France seconded the deputy branch head, who is a medical doctor and specialist in Epidemiology and Public Health in October 2010. Furthermore France is providing the ASTER NRT surveillance system free of charge for the DHSC.
Further nations, which indicated interest in active participation in the DHSC, include Austria, the USA and Poland. The support of additional nations and the timely manning of the vacant positions in the IT- and Operations Section are crucial in order to enable the DHSC to provide state of the art deployment health surveillance capabilities for NATO missions. Due to the still limited staffing of the DHSC, the NRT disease surveillance tool ASTER can currently not be provided for the support of the ISAF mission in Afghanistan.
DHSC current focus of work:

Continuous development and professionalization of the NRT surveillance system ASTER for multinational and NATO use is the first DHSC priority. For this purpose the DHSC has started an ongoing NRT surveillance project in Djibouti (DJI), East-Africa in February 2011. DJI was chosen because French, German and US troops are deployed in DJI and the NATO Maritime Operation OCEAN SHIELD is operating in the area. France is already operating ASTER in DJI since several years.
During a 2-weeks DHSC mission to DJI, an international team of experts (French, German, and USA) established an ASTER connection between the DHSC in Munich and the German medical Role 1 facility and the French medical Role 1 facilities in DJI.
Furthermore, the initial preparation for a future ASTER connection of the medical facility of the US Military Camp Lemonnier in DJI with the DHSC in Munich was accomplished by the expert team in cooperation with the US colleagues.
Another action point of the DHSC team in DJI was the establishment of initial contact with the liaison officer of NATO Operation OCEAN SHIELD in DJI, in order to identify possible ways for future DHSC support of this NATO maritime operation.
Since March 2011 the DHSC is continuously receiving and analyzing NRT surveillance data from the German and French medical Role 1 facilities in DJI. This enables the DHSC to continuously monitor and test NRT surveillance communication lines, feed-back mechanisms and compliance of the ASTER users.
The second focus of DHSC work is the improvement of the weekly NATO deployment health reporting tool EpiNATO. The EpiNATO reporting tool has been established in the NATO Implementation Force (IFOR) mission in Bosnia-Herzegovina 1996, following a British initiative. Since then its operational usefulness has repeatedly been questioned. Compliance of the users is weak and the absence of effective feed-back mechanisms seems to be a major cause for this.
In accordance with a decision of the COMEDS Force Health Protection Working Group (FHP WG), the DHSC has been tasked by NATO ACO to start an initiative to improve EpiNATO. The DHSC has initiated an EpiNATO stakeholder workshop in Munich in order to write a consolidated proposal for a thorough improvement of the EpiNATO tool, which has to be simple, efficient, relevant, mission oriented and above all operational. For that purpose the workshop participants will be tasked to revise the doctrinal background for EpiNATO (Allied Medical Publication-21) as well. As soon as the results of this workshop are endorsed by the FHP WG and NATO ACO, a DHSC mission to ISAF is envisaged in order to implement the improved EpiNATO version in ISAF.
Future DHSC development:
 Multinational team members at the
monitors
Multinational team members at the
monitors
Aiming at a better integration into the NATO architecture, a close connection of the Munich DHSC branch, which is still a structure of the German Bundeswehr Medical Office with the NATO Military Medical Center of Excellence (MilMed COE) in Budapest, was envisaged. This has been realized by fully integrating the DHSC as a Munich based satellite branch into the Budapest MilMed COE in 2011. Through this integration, a better connection with the NATO Command and Control architecture is granted.
When the final testing of the NRT surveillance tool ASTER in DJI will be successfully finished, the DHSC is aiming at deploying this early warning surveillance capability as soon as possible to ongoing NATO missions i.e. to ISAF in Afghanistan. This objective though will only be achievable, if a timely staffing of the vacant positions in the DHSC can be realized.
As a long term perspective, a step by step integration of-, and network creation with different- and multidisciplinary surveillance aspects like laboratory surveillance, veterinary surveillance, entomological surveillance and standardized coded surveillance, like the International Classification of Diseases (ICD 10) will make the DHSC a comprehensive and integrated deployment health surveillance tool for NATO.
As the “Comprehensive Approach” of NATO’s new strategy is aiming at a much closer and more intensive civil military cooperation and coordination, NATO’s military medical capabilities will closely cooperate with the civilian medical community. Therefore the DHSC is planning to integrate itself into a civil-military / national and international network of epidemiological competence centers. An initial working relationship has already been established with the German Robert Koch Institut (RKI) on the national side. Internationally, contacts of the DHSC with the World Health Organisation’s (WHO) Global Outbreak Alert and Response Network (GOARN) and the Epidemic Intelligence Section of the European Center for Disease Control and Prevention (ECDC) already exist.
On the military side, the intensive cooperation with the French Institut de Médecine Tropicale du Service de Santé des Armées (IMTSSA) and it’s successive organisation the Centre d' Epidémiologie et de Santé Publique des Armées (CESPA) will continue to be an essential paradigm of the DHSC. Furthermore the DHSC is planning to intensify the already very close and productive collaboration with the USA Armed Forces Health Surveillance Centre (AFHSC).
Conclusion:
The development process for the multinational NATO DHSC has been a success story. It showed that the concept of a multinational deployment health surveillance capability for NATO works. The DHSC approach has proven, that by integrating different national surveillance capabilities, the detection of disease outbreaks (naturally occurring or deliberately caused) can be accomplished quicker (better sensitivity) and more accurate (better specificity) than by purely national systems. Furthermore, the multinational DHSC concept of integration and burden sharing promises to be more cost effective than several national surveillance systems and concepts, which are running in parallel.
The mission of the DHSC is to contribute to a better preparedness of the deployed NATO Forces against the threats of infectious disease and bioterrorist attacks. Therefore the DHSC is supporting operational readiness of our soldiers in NATO deployments and strengthening the Force Health Protection efforts of the military medical services in NATO.
Date: 01/31/2019
Source: Medical Corps International Forum (4/2011)

