Article: H. CVITANOVIC, E. JANCIC, V. CVITANOVIC, V. VUKIC (CROATIA)
Organization and Military Medical Doctrine During the War Of Independence (1991-1995) In Karlovac County, Croatia
War conditions called for a military medicine that would integrate civil and military components. The General Hospital Karlovac, the medical corps of the Croatian Army, and emergency, preventive, and general medicine care were in cooperation and formed an integrated war health organization. The wounded from the battlefield of the Karlovac area were admitted to and treated at the General Hospital Karlovac, totaling 1475 wounded, 39 of whom died of wounds. 229 people killed in action were directly admitted to the Department of Pathology. The Medical Corps of the Croatian Army provided only primary health care services and emergency care. Due to the vicinity of the battlefield the classic echelon structure could not be followed in the Karlovac County. Civilian emergency, preventive, and general medical care facilities treated mostly civilians but in the beginning of the war also military personnel. The concept of collaboration between civilian and military medical services was successfully implemented in the Karlovac County, resulting in effective health care.
Introduction
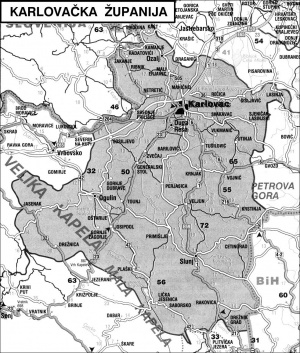 Map of Karlovac County.
Map of Karlovac County.
The Croatian War of Independence was fought from 1991 to 1995 between Croatian forces loyal to the government of Croatia and the Serb-controlled Yugoslav People's Army (JNA) al well as local Serbian forces. At the beginning of the war, the JNA tried to forcefully keep Croatia within Yugoslavia. After failing to succeed with this aim, Serbian forces established the self-proclaimed Republic of Serbian Krajina (RSK) within Croatia. After the ceasefire of January 1992 and international recognition of the Republic of Croatia the front lines were entrenched. The United Nations Protection Force (UNPROFOR) was deployed.In 1995, Croatia launched two major offensives known as “Operation Flash” and “Operation Storm” and finished the war with an overall victory achieving independence and preservation of its borders. After the war, Croatia was devastated, the economy destroyed with losses in damaged houses, infrastructure and refugee-related costs estimated at a total of $37 billion. The number of deaths on both sides was around 20.000 and there were refugees displaced on both sides. Karlovac County is a medium sized and relatively less densely populated county, covering 3644 sq. km., wiwth a population of 184,577 in 1991. The County has five cities (Karlovac, Ogulin, Duga Resa, Slunj, Ozalj) and sixteen (16) municipalities (Barilović, Bosiljevo, Cetingrad, Draganić, Generalski Stol, Josipdol, Krnjak, Lasinja, Netretić, Plaški, Rakovica, Ribnik, Saborsko, Tounj, Vojnić and Žakanje).Karlovac County is situated on the border between the Central Highlands of Croatia at the narrowest part of the national territory. The County borders with the Republic of Slovenia and the Republic of Bosnia and Herzegovina. Karlovac, capital of the county, was on the frontline during the war. More than 52% of county territory was temporarily occupied. Very important infrastructure, material and cultural goods were destroyed causing intensive migration and emigration trends. During the war, observation stations recorded a total of over 11.000 different caliber projectiles that fell on the town of Karlovac.
Organization of Wartime Health Care System by the Ministry of Health and General Staff of the Croatian Medical Corps
Our military medical doctrine was emerging along with the Croatian state and the army. Former Military Health of JNA (Yugoslav National Army) was hostile to Croatia and our state could not expect any support from their side but had to rely on its own strength, especially on experts from the Faculty of Medicine in Zagreb, who as heads of different departments of GSSRH (General Staff of the Croatian Medical Corps) led by Health Minister Andrija Hebrang, created a Croatian military medical doctrine. The organization had been adapted to the specific situation in Croatia, and an integral civil-military health care system was created. Each battlefield had its specificity and the system had to adapt to the tactical situation on the ground as well as to availability of personnel and equipment. With this article we intent to present the organization and some specifics on the battlefield of Karlovac considering the comprehensive warfare situation in Croatia.
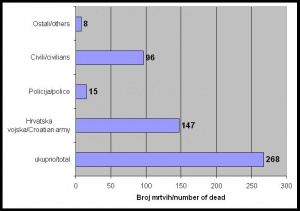 Number and distribution of Patients having died during treatment in General Hospital Karlovac
during the ware
Number and distribution of Patients having died during treatment in General Hospital Karlovac
during the ware
The development of the wartime health care system proceeded in three phases and on three levels of alert. The first MKE (mobile surgical teams) were set up, attributed to units of MUP (the Ministry of Internal Affairs) and located close to the battlefield in order to provide emergency medical care to wounded soldiers on the site of wounding and to provide psychological help as well. Apart from establishing MKE, reserves and maneuvering hospitals were adopted in this phase.
In late May 1991, the second phase was begun throughout the establishment of GSSRH. General Staff of the Croatian Medical Corps had a crucial role in the Croatian wartime health care system, from the development of logistics and coordination to the direct assistance on the field. The General Staff employed departments for wound care, preventive medical care, toxicology, military psychiatry, information and research, education, medical support to MUP, as well as the department of logistics, legal and economic affairs and the ethics committee. GSSRH elaborated the plans and preparations for state of war, which were based on the available sources of civilian health care resulting in all civilian hospitals near the battlefield becoming war hospitals;, as major hospital, or background war hospital, was determined one positioned far behind the line of fire. The evacuation plans were determined and the provisional surgical stations were organized. In June 1991, the collection and supply of war material and technical resources were intensified. Seminars of emergency war surgery were installed.
In August 1991, all necessary plans were completed and the first level of preparedness was inforced, including coordination between GSSRH and health care institutions along with permanent duty attendance. Secure storage areas for drugs and other medical supplies were provided and surgical teams and teams of general medicine were kept in stand-by. A list of all medications was drafted and implemented, and national drug manufacturers were put under a special regime.
All directors of health care institutions were subordinated, vacations were suspended. The evacuation plans for patients and institutions were established and the hygienic-epidemiological service was activated.
 Number of wounded treated in General Hospital Karlovac during war inKarlovac County and their
distribution.
Number of wounded treated in General Hospital Karlovac during war inKarlovac County and their
distribution.
GSSRH defined the second and third stages of readiness. In the second stage all necessary personnel were mobilized as well as drugs and medical supplies; a compact training for teams of the Red Cross was conducted, the work of voluntary blood donors was coordinated, etc. In the third stage of readiness, measures of organization and management required in the event of outright war were determined.
In early August 1991, the third phase of development of the wartime health care was initiated. The war activities were intensifying so that teams of general practitioners were included in the system, instant training was conducted and the system of improvised transport of the wounded was organized.
On 21 August 1991, all Croatian health care institutions were fully adapted to wartime conditions. In terms of the imposed war and the lack of a military medical corps, it became necessary to create war medical doctrine.
Unique war medical doctrine is the system of the basic principles by which physicians of a country are ruled in order to perform tasks of prophylaxis, treatment and organized medical care of the sick and wounded. The need for a unified action derived from the fact that any action has to be performed in very poor conditions while needing to provide care for large numbers of people with limited resources available; therefore doctors have to act in accordance with the most reliable and best methods of medicine which are available in this situation. Equally important is the fact that the patient encounters a large number of institutions and physicians with different approaches and medical backgrounds requiring, the establishment of a clear and common doctrine. Therefore, GSSRH had decided to prepare the so-called “NATO Handbook” in order to harmonize procedures and to improve healthcare in wartime conditions. The core feature of a doctrine is integration of civilian and military components along with comprehensive mobilization of all human and material resources with vertical subordination as well as parallel coordination of civil and military systems and the echelon system.
Related to the different conditions on the battlefield, three methods of medical care were identified. Special Forces were taken care of by surgical-anesthetic teams on the first and second echelon levels. In the besieged cities, the first echelon consisted of paramedics in the armed forces or members of civil protection, all other levels of care were carried out in civilian hospitals that had been rearranged into military hospitals in the first line of defense.
A classical echelon system was applied on the open battlefield. The first echelon consisted of trained nurses and physicians, and the second echelon was covered by battalion surgeons conducting primary surgical care. The third echelon's team of surgeons was at the brigade level enabling to perform a higher level of surgical care and prepare the patient for further transport. The civilian hospital near the front line was the fourth echelon of medical care. The fifth echelon’s hospitals were highly specialized clinical centers in the deeper rear area.
In order to come up with an effective organization, GSSRH appointed Commanders of Health Crisis Staff at the regional level (the county level) who then passed orders to the lower levels, such as the Crisis Centre of Health Facilities. The role of the Health Crisis County Centre was to coordinate activities to allocate human and material resources, to take over the management of the health care system in wartime or in imminent danger of war, to elaborate evacuation plans, to work out a backup location, to mobilize supplies, to fill up certain teams with personnel, to control and to introduce a mandatory work recording, especially for the wounded and dead, to coordinate activities with civilian and military authorities and to report all these activities. At the level of each institution a separate Crisis Staff was established. Its role was to implement decisions of the County Crisis Staff and GSSRH and to ensure the most effective work of the institution adapting to the tactical situation.
The organization of the War Health Care in the Karlovac War Zone
Before the beginning of the war, all health care institutions in Karlovac were merged in the Medical Center. Overall, there were 1515 employees, and the hospital provided 699 nursing beds. Health care units were deployed at 16 sites in the town of Karlovac. In the period from late August to December 1991, 449 employees had left the medical center including 60 doctors and 137 nurses. The loss of such a large number of medical personnel increased difficulties in preparing a health care system in warfare conditions.
 War destruction of General Hospital Karlovac.
War destruction of General Hospital Karlovac.
The organization of war health care in Karlovac was based on the Medical Center part of which was the hospital. The hospital was conducting the acceptance and treatment of the wounded along the line of battlefield in Karlovac County. The Medical Center was conducted by the Crisis Staff following the orders of the General Staff of the Croatian Medical Corps, the Ministries of Health and Defense. The Crisis Staff had developed plans in case of war on the local level and carried them out to the extent that required current development of tactical situations. In collaboration with the General Staff of the Croatian Medical Corps and the Ministry of Health and with local civilian and military authorities, the Crisis Staff ordered personnel to work in hospitals, carried out the re-staffing of personnel and the replenishment of material-technical assets of the mobile hospitals and performed exercises of mobilization. A plan of evacuation was elaborated, designated places for shelters and heightened security measures were defined.
Considering the organization, three basic components of war health care in Karlovac could be outlined. The first component was the General Hospital, the second the Military Medical Service, and the third was the provision of emergency, preventive and general medical care.
During the whole war, the General Hospital Karlovac was several kilometers removed from the first line of fire. This position required significant organizational and personnel changes and a great deal of effort by all employees during the war years.
Therefore, the hospital's work-time was adjusted in accordance with improvised facility conditions and the utilization of basement rooms. Functioning as the main evacuation hospital, due to the proximity to the battlefield it served at the same time as a triage station combining the second and third echelon of providing health care in war conditions.
Along with protective measures, reserve locations for hospital evacuation were provided, and all the material and technical conditions were secured. Shifts were in groups of 24 hours, continuously during the alert. For the entire time of intensive warfare actions, all services were on permanent duty. Equipment and personnel strength were satisfactory despite war damage of equipment and facilities, as well as the escape of a large number of employees on the enemy side. A big problem was that the hospital became a frequent target for hostile attacks, several times under heavy machinegun and mortar fire. Providing of medical care to the wounded was organized so that all wounded were coming to the emergency room where surgeons performed triage, and then either be processed and released to outpatient treatment or, depending on the patients’ status, be hospitalized and referred to the surgical department, right at the surgery or in the intensive care unit. After stabilization, the most seriously wounded were evacuated to the hospitals in in the rear area (in Zagreb and Čakovec) for further treatment.
Overall results of this approach were satisfactory because the centralization of the health care delivery system allowed the implementation of a unified medical doctrine for the treatment of the wounded. Numerically, this can be illustrated by a mere 8.2 percent of wounded who died in hospital out of all the wounded who had been admitted, which is consistent with results and experiences from other areas in Croatia affected by the war.
Beginning with the first casualties during the "Bloody Easter" in Plitvice on 31st March 1991, 1475 wounded had been treated in the General Hospital Karlovac by the end of the war. During the hospitalization, 39 people had died of injuries sustained in the war. Killed were 229, admitted to the pathology department.
Total demographic losses in the Karlovac County were: 540 members of the Croatian Army, 392 civilians and 469 members of the Serbian forces. During the four years of war, the General Hospital Karlovac functioned with the necessary modifications in the organization of work and allocation of manpower, despite the shelling and destruction of objects. The hospital was the main institution that united the second, third and fourth echelon of health care delivery and successfully completed all tasks.
The second component was the Military Medical Service, whose task due to the proximity to the battlefield was to provide care only at the first - and possibly the second - echelon as well as all procedures within the scope of primary health care at the battalion and brigade level. At the very beginning of the war, in spring of 1991, for the army’s purpose, a medical clinic was established in the old hospital in Dubovac, which task was to care for Croatian Army soldiers until November 1991 when the Military Medical Service of Croatian Army was fully formed.
 War destruction of General Hospital Karlovac.
War destruction of General Hospital Karlovac.
Due to the vicinity of the battlefield in Karlovac, there was not a classic organization of echelons, as opposed to other fronts in the Homeland War, but after first aid and evacuation from the zone of imminent firing, initially, further evacuation was conducted by HMP (Emergency Medical Services), later on by the military medical service with their vehicles. First aid stations had not been established at the battalion and brigade levels, so that doctors only provided emergency medical care and the evacuation of wounded was continued to General Hospital Karlovac.
In the further course of the war, a garrison clinic was established, and doctors were placed in battalions and brigades. Medical stations were foreseen at battalion and brigade levels, but due to the proximity of the hospital to the front line they had not been placed in function.
The Military Medical Service of 304th Logistical Base of Karlovac Corps established the ambulance station in the village Levkušje, with two medical teams composed of a doctor, two nurses and an ambulance driver with a motor vehicle.
As in other areas of battle in Croatia, the Military Medical Service in Karlovac played a small role in the treatment of the wounded, but rather concentrated on the evacuation to hospitals and the implementation of preventive and primary care of soldiers.
The third component was the provision of emergency, preventive and general medical care. The HMP (Emergency Medical Service) probably played a crucial role during the war because in addition to taking care of civilians, it provided initial evacuation from the front line. During the course of the war, the HMP was not only caring for the wounded, but had intervened in other emergencies, conducted home visits, transport of patients in the town area and evacuation to the background hospital. Also, the role of the MKE (Mobile Surgical Teams) operating in the beginning of the war at Topusko and Lasinja area should be mentioned. In Karlovac, due to the small depth of the battlefield, MKE were not activated during the most intensive combat in 1991. Later in the war, MKE had become integral parts of the Special Police Units, actively involved in the provision of medical care during the actions on other battlefields in Croatia.
In many cases, general practitioners were the first in the medical chain providing emergency medical care and, through their continuous 24 hours service at several locations in the town, relieved The HMP and the Military Medical Service while continuing to provided the usual health care for the civilian population.
This was also an important moral and psychological factor. In the villages around Karlovac, general practice medical clinics for some time served as the emergency medical service and as the second echelon.
In addition to teams of general medicine, services of epidemiology and toxicology provided preventive health care. They executed permanent control of microbiological safety in facilities for the preparation and distribution of food, control of water and ready meals, vaccinations and registration of infectious diseases. In addition, they monitored contamination of air, soil, water and clothing.
Due to the proximity of the hospital to the front line, the organization in the battlefield of Karlovac was specific without any classical structure of second and third echelon of medical care. A medical station at the battalion and brigade level had not been formed and patients were cared for by nurses or physicians at the first echelon and then immediately transported to the General Hospital Karlovac for definitive care.
The General Hospital Karlovac functioned as a war hospital, but due to the proximity to the battlefield, it also functioned as a triage station, uniting the second and third echelon of medical care delivery in war conditions. MKE had not been used at this part of the battlefield due to the proximity of the General Hospital, but MKE acted as support on other battlefields of Dubrovnik, Maslenica and Velebit region.
Conclusion
 Map with medical stations and hospitals.
Map with medical stations and hospitals.
The General Hospital Karlovac acted as a war hospital, but, due to its proximity to the battlefield, also as a triage station, uniting the second and third echelon of medical care delivery in war conditions. The hospital had been a pivot institution that faced aggression and yet successfully completed all tasks. The Military Medical Service worked closely with civilian health institutions, the evacuation was quick and efficient and the losses were minimized.
During the entire duration of the war operations, both, civilian and military components of the health care organization were successfully unified. Cooperation of all segments of the war health care in Karlovac County was adequate, and it can be said with certainty that the health sector had an important role in the defense and liberation of our homeland. The integral concept of health care during wartime and imminent danger of war proved to be effective.
Author:
LtC Veljko Vukic, MD, Senior Expert Advisor, Military Medical Service Department, MOD Republic of Croatia
Co-Authors:
MSc Hrvoje Cvitanovic, MD, spec. dermatovenerologist, Head of Department of Dermatology and Venereology, General Hospital Karlovac
Ervin Jancic, MD, spec. neurologist, Department of Mental Disorders, General Hospital Karlovac
MSc Prim Vladimir Cvitanovic, MD, specialist in general medicine (ret.)
Date: 03/11/2019
Source: Medical Corps International Forum (2/2013)