Article: C. CROSS
CANADIAN ARMED FORCES MEDICAL RISK MATRIX
From the CAF perspective, a stratified risk matrix was formulated by the Directorate of Medical Policy/Medical Standards, which balanced an acceptable level of risk to the health and safety of CAF personnel, whilst taking into consideration the potential unavailability of an appropriate level of medical care required, due to operational situation. The following article explains history and format of this matrix.
Introduction
The mission of the Department of National Defence and the Canadian Armed Forces (CAF) is to defend Canada and North America, their interests and values, while contributing to international peace and security. In order to meet these mission requirements, the CAF is given broad authority and latitude in utilizing CAF members, for which Section 33 of the National Defence Act is the statutory basis. The Act states that “The Regular Force, all units and other elements thereof and all officers and non-commissioned members thereof are at all times liable to perform any lawful duty”. Section 33 has similar requirements for the Reserve Force. This statutory requirement is the legal foundation for the Universality of Service principle, which states that “CAF members are liable to perform general military duties and common defence and security duties, not just the duties of their military occupation or occupational specification. This may include, but is not limited to, the requirement to be physically fit, employable and deployable for general operational duties”.
Generic task statements
These specific requirements of physical fitness, employability and deployability are codified in the Defence Administrative Orders and Directives (DAOD) 5023-0 and 5023-1, which define minimum operational standards, for which all CAF personnel are expected to meet. These generic tasks are based on the “soldier first” principle and require an ability to fulfill 6 common “bone fide occupational requirement” physical tasks and also to perform duties whilst deployed. The latter requirement include an ability to perform duties in a variety of geographical locations and climatic conditions in any physical environment, to deploy on short notice, to sustain irregular or prolonged working hours, ability to tolerate irregular or limited meals, travel as a passenger in any mode of transportation, perform duties under physical and mental stress, to perform duties with minimal or no medical support and also perform effectively without critical medication.
For those personnel who are unable to meet the generic tasks of Universality of Service, they will likely be released from the CAF, for which a decision is determined by the Directorate of Military Career Administration (DMCA), a non-medical CAF organization.
Determination of medical fitness
Medical fitness of personnel is determined by Canadian Forces Health Services physicians, utilizing occupational medicine principles and the CAF Medical Standards. The Directorate of Medical Policy/Medical Standards, has the delegated authority on behalf of the Surgeon General, to assign permanent change of medical employment limitations and medical category, in a fair and consistent manner. In 2008, it was recognized that a change in approach regards assessment of medical fitness of CAF member’s with complex medical conditions should be considered. This decision in part was related to the number of personnel who were being released and also influenced by the operational tempo requirements at the time, which was primarily focussed on the conflict in Afghanistan.
Medical risk matrix
From review of the medical literature at that time, it was recognized that some organizations were already utilizing a risk matrix stratification concept; this encompassed the probability of a medical condition recurring or exacerbating and the consequences of such an event, to include the requirement, type and degree of medical intervention required. This risk stratification concept was originally developed from an engineering perspective and was subsequently further developed as a tool and guidance for aeromedical decision-making related to astronauts who were being screened for International Space Station (ISS) duties. Similar risk matrices were developed for civil aviation and also for utilization by the CAF Aerospace and Undersea Medicine Board. Civil Aviation originally utilized a risk of 1 % per year, for which the probability of a catastrophic medical event being less or equal to this value, would be deemed unlikely to occur. These probabilities were further modified, dependent on the type of medical event and now utilize a risk tolerance of up to 2 % per year (20% per 10 year period).
From the CAF perspective, a stratified risk matrix was subsequently formulated by the Directorate of Medical Policy/Medical Standards, which balanced an acceptable level of risk to the health and safety of CAF personnel, whilst taking into consideration the potential unavailability of an appropriate level of medical care required, due to operational situation. In addition, it considers the potential effect of a medical event on an operational mission. However the acceptance of such risk, to include the probability of occurrences of medical conditions and consequences thereof, is a Chain of Command decision. In this respect, the CAF Armed Force Council, a General Officer forum, reviewed the original proposal and endorsed this approach.
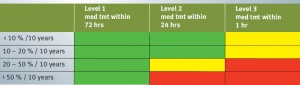
The finalized risk matrix approved, is now routinely utilized by D Med Pol/Med Stds, for review of appropriate medical cases, for which risk stratification can be applied. Its purpose is to translate medical employment limitations of CAF personnel with significant medical conditions into a stratified risk. Each determination is an individualized assessment utilizing up to date scientific evidence to predict the probable future recurrence of a medical condition, level of medical care required and associated operational consequences. The likelihood of recurrence is divided into four levels of risk, which are assigned over a 10 year time-frame, which are as follows: < 10 %/10 years, 10-20 %/10 years, 20-50%/10 years and > 50%/10 years. The severity of outcome is divided into three levels:
Level 1
- Adverse medical consequences are likely to cause physical or mental discomfort which would benefit from medical attention as soon as possible, but will rarely lead to long-term consequences.
- Adverse medical consequences are likely to cause some decrement in performance and a CAF member would benefit from being removed from duty; however the member would be able to remain on duty and perform the mission.
Level 2
- Adverse medical are likely to be in the form of an acute medical crisis. While immediate medical attention may not be crucial, lack of timely medical attention could lead to some long-term consequences.
- Adverse medical consequences are likely to cause moderate decrement in performance; however, will have difficulty fully safeguarding self and could be unfavourable to the mission.
Level 3
- Adverse medical consequences are likely to cause serious medical outcome to a CAF member, which could lead to serious outcome or serious permanent disability, if medical support is not immediate.
- Adverse medical consequences are likely to cause severe decrement in performance, as the member will be totally incapacitated and incapable of defending self; this will bring serious outcomes to the mission.
The risk stratification matrix is colour coded, in a Red/Yellow/Green “stop-light” format, for which a GREEN designation indicates a member has low medical risk within a military environment, for which a CAF member can contribute greatly with the assigned medical employment limitations. For a YELLOW designation, this indicates a CAF member would have a moderate medical risk within a military environment; however could contribute acceptably with assigned medical employment limitations. For a RED designation, this indicates a CAF member would have a high medical risk within a military environment. In such cases, caution should be taken when considering unrestricted retention in these specific medical cases.
Conclusion
D Med Pol/Med Stds utilizes the above risk stratification matrix for several medical conditions, some of which include seizure, traumatic brain injury, cardiovascular events (specifically personnel who have experienced a myocardial infarction), cerebrovascular accident, renal calculi and previous history of thromboembolic events. For such conditions, medical employment limitations which are assigned will include the probability of risk and level of medical care required and degree of incapacitation. This information is then evaluated by the Directorate of Military Career Administration, in order to determine if a member can be retained or should be released from the CAF. By utilizing this approach, medical employment limitations assigned provide a degree of flexibility for the Chain of Command to make appropriate and informed decisions, utilizing an individualized risk assessment for CAF members. This approach is both scientific and defendable; it also results in optimizing retention of trained experienced personnel, who would previously have been released from service, which is both advantageous to the member and the CAF.
Date: 04/18/2019
Source: Medical Corps International Forum (3/2015)