En Route Care (ERC) teams are pivotal to US military global patient movement and joint force sustainment, a role rendered even more urgent by the demands of Strategic Competition of Great Powers 30, 31. Despite their operational importance, assessment methods for ERC teams remain underdeveloped, inconsistently standardized, and lack robust validation. This systematic review synthesizes peer-reviewed, doctrinal, and grey literature (2003–2024), incorporating military guidance from the Joint Trauma System and US Department of Defense (DOD) to critically appraise all studies
Introduction
ERC teams serve as global lifelines for US and allied military personnel, providing advanced medical care in austere, high-threat environments where rapid stabilization and evacuation are required for mission success. Their proven effectiveness across the range of military operations has made them an indispensable joint force sustainment asset, yet their performance assessment frameworks have not kept pace with the evolving complexity of modern conflict 30, 31. The onset of Strategic Competition of Great Powers has further highlighted the urgent need for rigorous, standardized, and technologically integrated tools to continuously monitor ERC readiness and competency 1 -3, 29-31.
Despite longstanding recognition of ERC teams’ value, the literature reveals persistent gaps in documentation, feedback, and validation of team-based assessment tools. Existing methods, though foundational, often lack operational relevance and adaptability to unpredictable environments, limiting their utility for strategic planning and force sustainment. Accordingly, this review systematically synthesizes current frameworks and recent advances to determine how ERC performance assessments can better align with doctrinal guidance and emerging operational requirements, providing a blueprint for enhanced readiness in future military operations.
Methods
Study Identification and Screening Process
A systematic search was conducted across PubMed, CINAHL, Scopus, EMBASE, Cochrane, AFRL Technical Library, DOD E-Pubs, the Joint Trauma System Clinical Practice Guideline (CPG) repository, and DTIC, including literature published from 2003 to 2024. The search strategy employed key terms: (“en-route critical care” OR “aeromedical evacuation” OR “ERC team” OR “critical care transport”) AND (“team performance assessment” OR “competency evaluation” OR “teamwork measurement” OR “simulation” OR “non-technical skills”) NOT (“emergency department” OR “hospital” OR “ICU”). Filters were set to include only English-language, human subject studies within the specified date range 1 ,6, 7.
Manual review of additional sources included Air Force Instructions (AFIs), Air Force Manuals (AFMANs), technical and training documents, Joint Trauma System CPGs, and DTIC/AFRL technical reports, as well as reviewer-suggested grey literature (e.g., JTS ERC CPG, Marine Corps En Route Care System/ERCS) 10, 12.
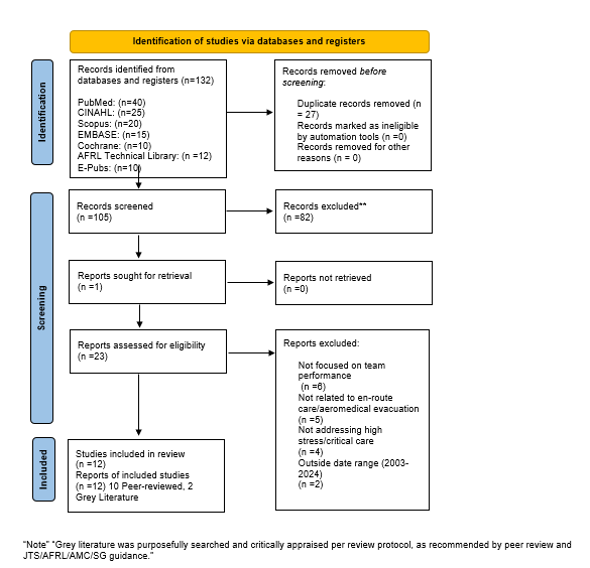
In total, 132 records were identified. After removal of duplicates (n=27), 105 unique records remained for initial screening. Title and abstract screening were conducted independently by two reviewers, with disagreements resolved by consensus, based on explicit inclusion and exclusion criteria guided by Joint Trauma System, AMC/SG, and DoD protocols 11. Articles not meeting inclusion criteria were excluded, with all exclusion decisions documented per Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines 27.
Results
PRISMA Flow Diagram
The results of this multi-stage screening are detailed in the PRISMA flow diagram (Figure 1), which quantifies records removed at each step and the reasons for exclusion, ensuring transparency and reproducibility throughout the selection process.
Study Characteristics
Table 1 presents design, sample size, quality ratings using the Mix Methods Appraisal Tool (MMAT), and key limitations for each included study demonstrating spectrum, methodological rigor, and operational context.
Appendix
- FFCCT: CRITICAL CARE AIR TRANSPORT TEAM
MET: CRITICAL CARE MEDICAL PERSONNEL PROVIDING OPERATIONAL SUPPORT FOR EN ROUTE CARE. TEAM PROVIDES ADVANCED MEDICAL CAPABILITY TO EVACUATE CRITICALLY ILL AND/OR INJURED PATIENTS REQUIRING SURGERY, RESUSCITATION, OR ADVANCED CARE DURING TRANSPORT. CCATT IS ASSIGNED OR ATTACHED TO AN AE EXPEDITIONARY ELEMENT AND BECOME AN OPERATIONS GROUP CAPABILITY WITHIN THE EXPEDITIONARY AE ELEMENT COMMAND STRUCTURE. CCATT, IN CONJUNCTION WITH THE EQUIPMENT PACKAGE UTC FFCC4, PROVIDES CARE FOR A MAXIMUM PATIENT LOAD OF UP TO 6 HIGH-ACUITY PATIENTS (IF TEAM COMPOSITION IS AUGMENTED WITH AN ADDITIONAL NURSE), OR UP TO 6 LOWER-ACUITY, STABLIZED PATIENTS; LOADS ARE DEPENDENT ON PATIENT ACUITY LEVELS AND TEAM AUGMENTATION STATUS.
- OPR: AMC/SGK
- OCR: AMC/SGX 12 Aug 2024
- PERFORMANCE MEASURES/SAMPLES OF BEHAVIOR
STANDARD MEASURE
- YES/NO CORRECTLY PRE-FLIGHT AND OPERATE MEDICAL EQUIPMENT IAW AFMAN 10-2909 AND THE AE EQUIPMENT COMPENDIUM OR AS REQUIRED BY MISSION PARAMETERS.
- YES/NO ALL PERSONNEL MAINTAIN INDIVIDUAL AND UTC READINESS REQUIREMENTS IAW AFI 41-106 DAFI 48-107, VOLUME 2 AND AFTTP 3-42.51.
- YES/NO UTC MEMBERS HAVE BEEN ISSUED PROPER INDIVIDUAL PROTECTIVE CLOTHING AND EQUIPMENT FOR FLIGHT OPERATIONS IAW DAFI 48-107, VOLUME 2.
- YES/NO ALL UTC TEAM MEMBERS TRAINED ON AIR FORCE TACTICS, TECHNIQUES AND PROCEDURES (AFTTP)
3-42.51, CRITICAL CARE AIR TRANSPORT TEAM; AND ARE FAMILIAR WITH AIR FORCE TACTICS, TECHNIQUES AND PROCEDURES (AFTTP) 3-42.5, FAMILIARIZATION WITH AEROMEDICAL EVACUATION (AE) OPERATIONS PROCEDURES; AFMAN 11-2AE V3, AEROMEDICAL OPERATIONS AND DAFI 48-107, VOLUMES 1, 2, 3, AND 4. - YES/NO REVIEW FLIGHT CREW INFORMATION FILES (FCIF) AND SQUADRON READ FILES PRIOR TO EACH MISSION.
- YES/NO DURING PRE-FLIGHT PLANNING, CORRECTLY CALCULATE AND PROPERLY COORDINATE POWER REQUIREMENTS INCLUDING CONSIDERING POTENTIAL MISSION DELAYS AT THE FLIGHT LINE, DURING GROUND TRANSPORT, AND FOR PATIENT EMERGENCIES. COMMUNICATE THESE REQUIREMENTS TO THE MCD.
- YES/NO DURING PRE-FLIGHT PLANNING, CORRECTLY CALCULATE AND PROPERLY COORDINATE OXYGEN REQUIREMENTS INCLUDING CONSIDERING POTENTIAL MISSION DELAYS AT THE FLIGHT LINE, DURING GROUND TRANSPORT, AND FOR PATIENT EMERGENCIES. COMMUNICATE THESE REQUIREMENTS TO THE MCD.
- YES/NO DURING PRE-FLIGHT PLANNING DETERMINE MEDICATION AND FLUID REQUIREMENTS FOR TRANSPORT; ENSURE THAT APPROPRIATE SUPPLIES ARE PROCURED FROM THE SENDING MTF OR OTHER RESOURCES.
- YES/NO PACKAGE AND MAINTAIN AUTHORIZED EQUIPMENT AND SUPPLIES IAW UTC FFCCA – 887N ALLOWANCE STANDARD.
- YES/NO DEMONSTRATE PROPER PROCEDURES FOR SECURING ALL EQUIPMENT, TO INCLUDE SPARE EQUIPMENT.
- YES/NO DEMONSTRATE USE OF PROPER SAFETY PRACTICES. EXAMPLES INCLUDE: 1) REMOVAL OF RINGS; 2) WEARING GLOVES WHILE LOADING AND UNLOADING LITTERS AND EQUIPMENT; 3) USE OF GOGGLES DURING ENGINE-RUNNING ONLOAD/OFFLOAD (ERO); 4) REMOVAL OF GLOVES WHEN HANDLING OXYGEN; 5) FAMILIARITY WITH GROUND OPERATIONS INVOLVED IN LAUNCH AND RECOVERY, BASIC FLIGHT LINE SAFETY, I.E. CIRCLE OF SAFETY, FOD AND THE DIFFERENCES INVOLVED IN A TACTICAL ENVIRONMENT; 6) COLLABORATION NOTED BETWEEN CCATT AND AECMS AS NEEDED DURING GROUND OPERATIONS; 7) CCATT DUTY/REST GUIDANCE IN DAFI 48-107, VOLUME 2 IS FOLLOWED.
- YES/NO UTC MEMBERS ARE TRAINED AND ABLE TO ENSURE AIR FORCE INSTRUCTIONS AND SAFETY STANDARDS ARE FOLLOWED DURING ENPLANING/DEPLANING PATIENTS, VEHICLE MARSHALLING AND REFUELING PROCEDURES.
- YES/NO DESCRIBE THE PROCEDURES FOR SAFETY DURING ERO (FIXED/ROTOR); APPROPRIATE PERSONAL PROTECTIVE EQUIPMENT.
- YES/NO DEMONSTRATE DOCUMENTATION OF PATIENT CARE UTILIZING THE AF FORM 3899L; EN ROUTE CRITICAL CARE FLOW SHEET.
- YES/NO DEMONSTRATE UNDERSTANDING OF PROPER COMMAND AND CONTROL NOTIFICATIONS AND DOCUMENTATION REQUIRED IN THE EVENT OF A MEDICAL EMERGENCY OR PATIENT STATUS CHANGE IN-FLIGHT.
- YES/NO DEMONSTRATE OR VERBALIZE BASIC KNOWLEDGE OF THE FOLLOWING AE EQUIPMENT: THERAPEUTIC LIQUID OXYGEN UNIT (PT LOX); UNITRON/FREQUENCY CONVERTER.
- YES/NO VERBALIZE IN-FLIGHT INFECTION CONTROL PROCEDURES; STANDARD PRECAUTIONS; KNOWLEDGE OF AFI ON INFECTION CONTROL, AECP FOR HEALTHCARE WORKED EXPOSURE TO BLOOD AND BODY FLUIDS AND CONTROL BIOHAZARDOUS WASTE IAW THEATER GUIDELINES. 
- YES/NO RESPOND APPROPRIATELY DURING IN-FLIGHT AIRCRAFT EMERGENCY.
- YES/NO DEMONSTRATE KNOWLEDGE OF EMERGENCY PERSONAL OXYGEN SOURCE(S) AND HOW TO DON, OPERATE, ETC.
- YES/NO VERBALIZE PROPER CLEANING AND DISINFECTING OF PMI PER MANUFACTURER’S RECOMMENDATION.
- YES/NO VERBALIZE PROCESS FOR REPORTING AND REPLACING BROKEN OR DAMAGED PMI IAW DAFI 48-107, VOLUME 1.
- YES/NO AT MISSION COMPLETION, STORE/SECURE MEDICAL EQUIPMENT AND KITS, RE-STOCK USED ITEMS, RE-PACK ALLOWANCE STANDARD, AND PLUG IN PMI.
- YES/NO VERBALIZE AND DEMONSTRATE KNOWLEDGE OF CONTROLLED SUBSTANCE DOCUMENTATION FOR EACH PATIENT AND FOR A MISSION IAW DAFI 48-107, VOLUME 1 & 2.
Personnel assigned will be current in the respective AFSC CMRP skills for the position they fill in the UTC. CMRP requirements must be accomplished IAW AFI 41-106, Air Force Medical Readiness Program.
Mit WhatsApp immer auf dem neuesten Stand bleiben!