Article: H. M. TAYSEIR A. MA’AWIA (SUDAN)
Massive subdural hematoma complicating severe falciparum cerebral malaria
Malaria remains a major killer disease in the tropics claiming more than one million lives annually in sub-Sahara Africa alone.
P. falciparum causes the most severe form of malaria associated with serious complications, which often prove fatal.
In this study, we present a rare case of subdural hematoma as complication of malaria falciparum.
Case presentation
An 18 years old male from central Sudan who is Shepard by profession presented to the casualty and emergency department with altered consciousness level. He had a history of fever for five days.
Fever:the condition started five days prior to admission with intermittent fever of moderate to high grade, associated with irritability without convulsions or loss of consciousness.
The patient consulted a doctor in the rural primary health care center who made the diagnosis of falciprum malaria based on positive blood film. Subsequently the patient was started on injectable artemether. He completed the prescribed dose in the same day of admission to our hospital.
Coma:the patient level of consciousness started to deteriorate few hours before he was admitted to the hospital. By the time he reached the casualty he was unconscious.
No history of trauma
There was no significant medical, drug or family history.
Clinical examination: the patient was unconscious, febrile, looked unwell and sleepy. He was not pale, jaundiced or cyanosed.
Vitals: pulse: 60/min, B.P. 130/80 mmHg, RR 16/min.
CNS: patient unconscious, not oriented to time, place or person. G.C.S.: 8
CVS, chest and abdomen: no abnormality
A clinical diagnosis of cerebral malaria was made and the patient was started on i.v. quinine 600mg TDS. He responded well to treatment and his coma scale reached 13 after the second dose of quinine. Upper and lower limbs were moving equally, power grade: 5. No sensory loss. No signs of meningeal irritation.
The patient’s condition remained static for three days. On his fourth day in hospital, the level of consciousness dropped again to reach GCS 5, associated with features of Rt. III cranial nerve palsy and increased reflexes in the right side.
At this stage, a CT scan of the brain was requested
Investigations
BFFM: Ring stage falciparum malaria (+++)
TWBC: 10,000 /cumm
Random blood glucose: 120 mg/dl
HB: 75%o
WIDAL test for enterica: Not suggestive
CT SCAN OF BRAIN:massive subdural hematoma extending from frontal to parietal region shifting from the mid line to the left
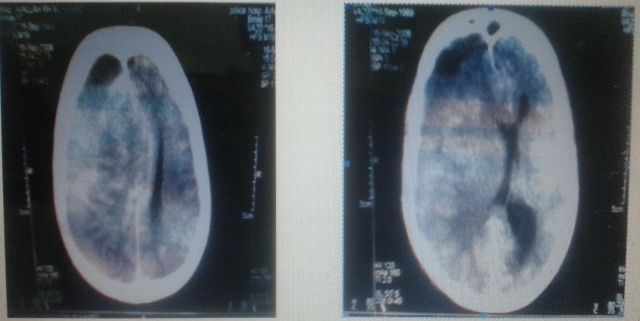 Fig. 1
Fig. 1
Management:
After receiving the CT scan report, it was obvious that the patient needed surgical care. The duty doctor in the dept. of neurosurgery was
Consulted. He advised emergency evacuation of the subdural haematoma as a life saving procedure.
The patient was immediately taken to theatre where the subdural haematoma was evacuated through a burr hole. A drain was fixed and the patient over hydrated for 24 hours post operatively to facilitate expansion of the brain.
He responded dramatically and regained his consciousness 12 hours after surgery.
The patient was kept on oral quinine and antibiotics. He was discharged in good condition on the third postoperative day.
Discussion
Bleeding and coagulation abnormalities are seen in less than 5% of patients with severe falciparum malaria. It can be due to thrombocytopenia and/or disseminated intravascular coagulation.
Mature parasitised red cells and cytokines activate the coagulation cascade. Accelerated coagulation cascade, consumption of anti
Massive thrombin III, increased concentration of FDP and increased spleenic clearance of platelets contribute to the coagulopathy and thrombocytopenia in malaria. Hypofibrinogenemia due to DIC occurs in 5% of patients.
Thrombocytopenia is commonly seen in severe falciparum malaria. It is presumed to be due to increased consumption of the platelets in the periphery, perhaps in the spleen. Bone marrow shows appropriate megakaryocyte response. However, bleeding due to thrombocytopenia is very rare in malaria. Corticosteroids are not indicated. However, if thrombocytopenia is severe, platelet transfusion may be considered. Generally, the platelet count returns to normal with the completion of antimalarial chemo therapy.
Disseminated intravascular coagulation is seen in less than 5% of patients with severe falciparum malaria. It tends to be more common in patients with cerebral malaria, pregnancy and secondary bacterial infections. D.I.C. in turn may aggravate the other complications of malaria like cerebral malaria, renal failure, pulmonary oedema and anemia (due to bleeding). Since it is rare, routine use of drugs like heparin may cause more harm than good and should be avoided. Prolonged prothrombin and partial thromboplastin time suggests the possibility of D.I.C. which can be confirmed by measuring plasma concentrations of fibrinogen and fibrin degradation products. D.I.C. in malaria has to be differentiated from that caused by many other conditions like heat stroke, viral haemorrhagic fevers, snake bites, immune complex disorders and shock. Treatment involves administration of fresh whole blood or fresh frozen plasma and injection of Vitamin K 10 mg intravenously. If there is fear of fluid overload, then exchange transfusion with fresh blood can be tried. Drugs that may cause gastrointestinal bleeding (aspirin, other NSAIDs and steroids) are better avoided in patients with severe malaria.
CONCLUSION
Subdural hematoma is a rare complication of falciparum malaria that needs urgent life saving surgical intervention. Therefore, it is wise to request a C. T. scan of the brain for malaria patients with deteriorating level of consciousness, especially when this is associated with neurological signs.
Authors
Lt. Col. (MC), Sudanese Armed Forces
General surgeon, Omdurman
Military Hospital
Graduated (MBBS) from Dr.Ambedkar Medical College,
Bangalore University, India
MD (GENERAL SURGERY), Gezira University, Sudan
E-mail: [email protected]
First and corresponding author
Date: 05/06/2015
Source: MCIF 2/15


