Report: R.MUHAMETI, L.NIKOLLARI (ALBANIA)
Beginning Tracheal Stenosis after Prolonged Intubation
Case Studies - Case 1, Tracheal Stenosis
Prolonged endotracheal intubation may lead to alteredtracheal blood flow, resulting in mucosal injury and scarringfollowed by tracheal stenosis. We report a case of the tracheal stenosis after prolonged endotracheal intubation from balloon cuff pressures. In this case study, we provide endoscopic images and descriptions of the bronchoscopy findings along with a brief discussion of the management for this complication.
Introduction
Tracheal Stenosis is a condition where the windpipe (trachea) narrows or becomes constricted (stenosis). When you breathe in through your nose or mouth, air travels down your throat (pharynx) and through the voice box (larynx). Air then travels through the largest airway, the windpipe. The windpipe has springy hoops of a tissue called cartilage in it, which keeps it open while you breathe. The windpipe branches into two smaller airways called the bronchi, which lead to the two lungs.
The entrance to the voice box (larynx) is covered by a small flap of tissue called the epiglottis, which automatically closes when we swallow to stop food or drink from entering the airways. In the voice box, there are two vocal cords (or vocal folds), with a space between them, which is called the glottis. If you have a sub-glottal stenosis, this means that the narrowing in your windpipe is below the glottis, so it is below your vocal cords. Supra-glottis means above the glottis, so if you have a supraglottic stenosis, it is higher up, above the larynx.
There are several different types of tracheal stenosis. These can be divided in to stenosis conditions that are present from birth (congenital), and acquired conditions, which have developed later in life. Causes include conditions resulting from treatments such as: endotracheal intubation, tracheostomy, radiotherapy or past surgery; external injury; cancer; and/or autoimmune conditions such as: polychondritis, sarcoidosis or Wegener’s granulomatosis.
It is important to note that some patients with a tracheal stenosis do not exhibit any symptoms while others may have one or more of the following symptoms: shortness of breath, coughing, wheezing, difficult or laboured breathing (dyspnoea), a breathing noise that is louder and harsher than a wheeze in someone with a windpipe or voice box obstruction, a bluish colour in the skin or mucous membranes such as in the mouth or nose and/or frequent lung inflammation.
Prolonged endotracheal intubation may lead to altered tracheal blood flow, resulting in mucosal injury and scarring followed by tracheal stenosis. We report a case of the tracheal stenosis after prolonged endotracheal intubation from balloon cuff pressures. In this case report, we provide endoscopic images and descriptions of the bronchoscopy findings along with a brief discussion of the management for this complication.
Case History
 Fig 1: Severe Tracheal Stenosis (Web-Like Stenosis)
Fig 1: Severe Tracheal Stenosis (Web-Like Stenosis)
A 45 year-old man was admitted in our clinic 2 month after an accident from a land-mine at the border between Albania and Kosovo. The patient’s hospital course was complicated by limited neurologic recovery, aspiration pneumonitis, and adult respiratory distress syndrome requiring an extended period of mechanical ventilation. At the first presentation he suffered from coughing, moderate dyspnoea and malaise. Flexible bronchoscopy was performed, first from above the tracheostomy revealing leakage of air bubbles from around an inflated cuff with underlying granulation tissue. Erosion of the mucosa overlying the tracheal rings was visualized in the region where the balloon cuff hadbeen positioned
(Fig. 1). After 21 days, the patient showed serious tracheal stenosis – an indication for tracheal dilatation or stent.
He had severe dyspnoea, stridor and moderate chest pain.
Follow-up bronchoscopy revealed severe damage of the tracheal lumen associated with web-like stenosis – which was treated by emergency tracheal stent (Fig.2).
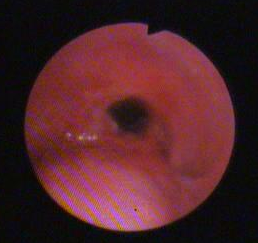



Fig 2. (After treatment with stent)
DISCUSSION and CONCLUSIONS
Although by placement of a balloon cuff a tracheostomy can provide an airway seal and thus prevent micro aspiration of oropharyngeal secretions and loss of tidal volume in ventilated patients, this measure is not without risk for complications. Specifically, patients with cuffed tracheostomy tubes are at risk for complications of balloon over-inflation resulting in elevated cuff pressures. These complications include ischemia and pressure necrosis, formation of tracheal wall defects, tracheomalacia, airway stenosis, and growth of granulation tissue. There are differing opinions about whether the injury is related to amount of cuff pressure or length of time the inflated cuff is in direct contact with the trachea. Pressures above this level have been shown to impair capillary perfusion in tracheal mucosa. In the case presented, we hypothesized that the aetiology of the complication described was multifactorial in nature, resulting from inadequate monitoring of the cuff pressure over an extended period of time and in the timeframe after the repair of a traumatic injury.
This bronchoscopic image re-enforces the importance of monitoring and maintaining of the trachea in patients with intubations for a prolonged period.
Reference:[email protected]
Authors
Colonel Rushan Muhameti, MD
Chief of Pneumology, Military Hospital Albania Armed Forces (AAF)
Tirana-Albania.
Address of the author:
Spitali Ushtarak, Rruga “Lord Bajron” Laprakë, Tirana-ALBANIA
Tel/Fax 00355 4223 3107
E-mail: [email protected]
First and corresponding author
CV
Rushan Muhameti was born in Erseke-Albania, 10 June 1967
He graduated from the faculty of medicine, GP branch in Albania in 1990. Specialized and graduated in pneumology in 1991 -1993 in the Institute of Pneumology in Albania. He completed his specialization at the Navy Hospital Athens, Greece for bronchoscopy Respiratory Lab., thoracoscopy,CT-imaging of Cancer.
⦁1990-1991 GP Civil Hospital Erseka-Albania
⦁1991-1993 Chief ofInfantry brigade Erseka
⦁Since 1993Physician pneumologist at Military Hospital Tirana-Albania
⦁Since 2008 Chief of Pneumology Military Hospital, Tirana-Albania
Co-Author:
Colonel LuanNIKOLLARI, PhD, Epidemiologist
Director Medical Military Institute
Central University Military Hospital
Date: 04/04/2015
Source: MCIF 2/15


