Article: Corresponding Author: Martin CM Bricknell
Maritime military medical response to the Mediterranean migration crisis: A scoping study
During 2015 and 2016, Europe experienced a period of increased irregular immigration predominantly across the Mediterranean to its southern coastal borders. Many stakeholders were involved in the maritime response to this phenomenon, conducting search and rescue (SAR) and border security activities. However, relatively limited literature exists on the role of the military in SAR activities and in the maritime health response. This article aims to report a scoping review of existing literature on the role of the military in the maritime medical response to irregular Mediterranean migration. Three electronic databases, Google scholar, and three non-indexed journals were searched, retrieving 629 articles of which 8 met the inclusion criteria for this study. This study found that all military maritime medical interventions were contextualised through discussion of relevant international legal obligations and were actualised through extensive inter-stakeholder collaboration. Further, it displays the tensions between humanitarianism and security in the development and framing of military operations capable of providing maritime medical care. Finally, this study highlights the diversity of health issues faced by people rescued at sea and the need for specific SAR vessels to address these acute health concerns. Several gaps in the literature are identified by this scoping study that necessitate further research. Specifically, exploration into the mediators of successful inter-stakeholder collaboration are recommended.
1. INTRODUCTION
In the past twenty years, the estimated population of international migrants has increased from 150 to 272 million people [1]. International migration is a global reality that will likely only increase as globalisation deepens, conflict, violence and economic desperation drive people from their homelands, and extreme weather events caused by global warming trigger mass displacement [1]. While the majority of international migration occurs within low and middle-income countries (LMIC), discourse on the topic focuses heavily on migration from LMICs to high-income countries (HIC) [2]. In Europe, migration has become an extremely contentious issue, particularly in the wake of a period of mass irregular immigration that peaked in 2015. This period, commonly referred to as a migration crisis, saw more than 1 million people arrive in Europe by irregular means across its land and sea borders [3]. This article will address this period of irregular immigration to Europe across the Mediterranean, the so-called Mediterranean migration crisis. The nationalities of migrants that crossed the Mediterranean in 2015 and 2016 are extremely diverse. The top 5 countries of origin were Syria, Afghanistan, Iraq, Nigeria and Eritrea [4]; all of these countries have experienced protracted conflict, instability, and displacement. The motivations of migrants for undertaking the perilous journey across the Mediterranean are diverse, and include fleeing conflict, violence, political insecurity and economic desperation. It is important to note that there are often multiple, inter-related motivations for migration and, as such, caution should be exercised when using nationality as a shortcut to assess the validity of these motivations [5]. Irregular migration across the Mediterranean occurs along three primary routes; the western route from Morocco to Spain, the central route from North Africa, particularly Libya, to Italy, and the eastern route from Turkey to Greece [6]. These pathways for irregular migration are extremely dangerous as human smugglers overload unseaworthy boats and dinghies with passengers. Such practices resulted in the deaths of more than 5,000 people in 2016 alone [7]. The massive death toll of irregular migration across the Mediterranean is not limited to the peak of the Mediterranean migration crisis in 2015 and 2016. Between 2000 and 2017, more than 33,000 people died or went missing on this journey [6]. As such, routine response mechanisms were already in place to reduce the loss of life at sea, and additional efforts were introduced in response to the unprecedented scale of the crisis. National coastguards of coastal states such as France and Italy have played a long-standing role in the humanitarian response to irregular migration across the Mediterranean [5]. In response to more recent influxes, nongovernment organisations (NGOs) including Save the Children, Medecins Sans Frontiers (MSF), Sea-Watch and SOS Mediterranee have also become important stakeholders [7]. On the supra-national level, the European Union (EU) is a key stakeholder, particularly following the creation of Operations Triton and Sophia, and additionally, the North Atlantic Treaty Organisation (NATO) through its cooperation with Frontex [8].
A large body of published literature discusses the role of NGOs in the maritime response to the Mediterranean migration crisis and their role in providing care to migrants at sea and upon arrival in Europe. In contrast, the literature discussing the role of military forces and personnel within national, EU and NATO operations in the provision of care to migrants rescued at sea is relatively limited. This paper addresses this gap by reporting a scoping study of existing literature on the role of the military in the maritime medical response to irregular Mediterranean migration. While irregular migration across the Mediterranean is no longer at the heights reached in 2015-2016, migration is a central feature of the 21st century that will require continued attention and response. Knowledge on the roles of diverse stakeholders in response to mass migration events is essential to improve future responses and inter-stakeholder collaboration.
2. METHODOLOGY
2.1 Identifying the research question
This scoping study aims to identify and map the role of military forces in maritime medical interventions for migrants during the Mediterranean migration crisis. The research question guiding this study is: ‘What was the role of military forces in the maritime medical interventions for migrants during the Mediterranean migration crisis?’ The term Mediterranean migration crisis is used to refer to the dramatic increase in boat migration to Europe that peaked in 2015. For the purposes of this review, maritime medical interventions include any medical care provided at sea by any military organisation or utilising any military infrastructure or personnel (e.g. national and EU military and naval forces). This scoping study has been conducted by drawing on the methodological framework developed by Arksey and O’Malley [9] and the subsequent recommendations for enhancement made by Levac, Colquhoun and O’Brien [10].
2.2 Search methods/identification of relevant studies
As scoping reviews are intended to be a comprehensive means of mapping a field of literature, Arksey and O’Malley [9] recommend conducting searches for literature using diverse sources such as electronic databases, reference lists, key journals, and relevant organisations and conferences. Meanwhile, Levac and colleagues [10] acknowledge that researchers must balance between breadth, comprehensiveness and feasibility, recommending that concerns for feasibility must not compromise the ability of the study to answer the research question and that researchers must justify decisions to limit the scope of their study. Decisions regarding languages of literature to be included and timespan of coverage should also be made at this stage [9]. For the purposes of this review, electronic databases were searched for relevant published academic literature and grey literature. Electronic databases searched for this review are: PubMed, SCOPUS, Medline. GoogleTM scholar searches were also conducted to identify further grey literature. Only literature in English published between 2015 and 2020 was included due to the language abilities of the authors and the timeframe of the migration patterns in focus. According to the framework employed, search strategies should be developed using the research question and the definitions of its key concepts [9]. As such, search terms were identified by extracting key terms from the research question.
Table 1: Search Strategy Military Medic* Mediterranean “refugee crisis” |
2.3 Study Selection
Arksey and O’Malley’s [9] framework recommends developing inclusion and exclusion criteria after the initial search of the literature so that relevance can be determined based on increased familiarity with the literature. Levac and colleagues [10] highlight that this is an iterative process which should be refined and conducted through reviewing abstracts and then, where necessary, full articles to determine relevance. Following the search of the literature using the search strategy outlined above, the following inclusion and exclusion criteria were developed:
Table 2: Inclusion and Exclusion Criteria Inclusion criteria Articles were included if: - Specifically addressed the health and medical components of maritime interventions directed at migrants crossing the Mediterranean - Health interventions addressed were provided between rescue at sea and delivery to reception centres on land Exclusion criteria Articles were excluded if: - They focused on health interventions delivered outside the Mediterranean - Studies about maritime health response in the Mediterranean, but focused on NGO or commercial activities |
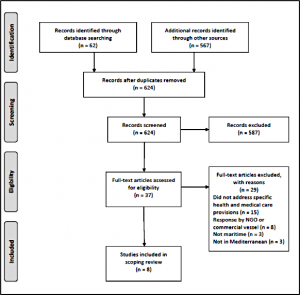
The initial literature search yielded 3,920 papers on GoogleTM scholar, of which the first 100 when sorted according to relevance were considered. 62 search results were drawn from the databases searched. Repetitions of results between sources were excluded. The available abstracts of all identified literature were first read and inclusion and exclusion criteria applied. Then, where abstracts were unavailable or did not provide clarity regarding relevance, the whole article was read and assessed for relevance using the inclusion and exclusion criteria. In addition to searching databases and GoogleTM scholar, three relevant non-indexed journals were hand searched; the International Review of Armed Forces Medical Services; Military-medicine.com; Journal of the Royal Naval Medical Services. Three relevant articles were found in the Journal of Royal Naval Medical Services.
2.4 Data extraction
Data was first extracted from the included sources using a table similar to that in the Arksey and O’Malley [9] framework. The titles of the table were: Authors, year of publication, study location; study type; study objectives; methodology; outcome measures; important results; key themes. All articles were then read with attention to the key themes and issues that arose. These themes were tabulated (see Table 3) and key sections of the sources that discussed these themes were organised in a Microsoft Excel document. The table of key themes was created iteratively, with new themes and issues being added with each article.
2.5 Reporting
Due to the diversity of the sources included in this literature review, focus on the common themes between them was deemed the most insightful way to approach reporting on the body of literature. The key themes drawn from the literature included are illustrated in Table 3 in the results section of this paper.
3. RESULTS
3.1 Overall findings
Figure 1 is a PRISMA Flow Diagram that represents the process of source selection for the study [11]. A total of eight sources were identified for inclusion in this scoping study. Five of these sources directly address the maritime medical response of the military in the Mediterranean migration crisis. Three of these studies were written by Surgeon Commanders in the UK Royal Navy and discuss the UK’s naval contributions to the maritime medical response [12, 13, 14]. The other two address medical treatment provided on board German and Irish naval vessels, respectively, and are also written by military doctors [15, 16]. The remaining three sources take a broader perspective on search and rescue (SAR) practices and their political contexts and controversies, addressing military maritime medical response as a brief component of these wider topics. Llewellyn’s [17] report on SAR practices in the Canal of Sicily was written in cooperation with migrants’ rights organisations and highlights the diversity of actors involved in SAR during the Mediterranean migration crisis. Patalano [18], a UK based academic, focuses on the Italian Mare Nostrum operation, while Panebianco [8], an Italian academic, contextualises this same operation within broader Italian and EU politics. These sources include a range of countries whose naval and military forces were involved in the provision of medical care during the maritime response to the Migration crisis.
3.2 Key Themes
Due to the diversity of these sources in their content and approach, the remainder of this results section will be structured around key themes arising in this body of literature (see Table 3).
Table 3: Key Themes
| SOLAS and | Operational
| Security vs.
| Inter-stakeholder
| Inter-stakeholder
| Health of
| Medical |
Geraghty |
|
|
|
|
| X | X |
Henning et. al., | X |
|
|
|
| X | X |
Hillman et. al.,(2017), UK naval ship used in Aegean Sea | X |
|
|
|
|
| X |
Kulla et. al.,(2016), German naval ship in Mediterranean delivering rescued people to Italy |
|
|
|
|
| X | X |
Llewellyn (2015), written In collaboration with migrants’ rights groups about SAR in Sicily, Italy | X | X | X | X | X |
|
|
Patalano(2015), about Italian context; UK based author | X | X | X | X |
|
|
|
Panebianco (2016), Italian academic on Italian context | X | X | X | X | X |
|
|
Sharp et. al., (2019), UK operation in Mediterranean | X |
|
| X |
| X | X |
3.3 Safety of Life at Sea and international law
A large body of international conventions legislates the duty of ships to render assistance at sea. Except Kulla et. al. [15] and Geraghty [16], every source identified by this scoping study references these conventions, applying them to contextualise the military responses they describe. Llewellyn [17] provides the most in depth discussion of relevant international law, describing the responsibilities of states as set out in United Nations Convention on the Law of the Sea of 1982 (UNCLOS), the International Convention on Maritime Search and Rescue of 1979 (SAR Convention), the Geneva Convention of 1951, and the Safety of Life at Sea (SOLAS) Convention. According to this body of international law, flag ships and commercial ships are required to provide assistance to any ship in distress within their vicinity, states are required to coordinate SAR efforts within their designated zone and provide places of safety for those rescued, and rescued migrants cannot be returned to territories where their life or freedom may be put in danger due to their religion, race, political opinion or nationality (non-refoulement). Henning et. al. [12] provides further detail specific to the SOLAS convention, stressing that in many places SOLAS has been ratified into national law, making a breach of the principles a criminal offence. They additionally highlight that the SOLAS convention requires the construction, equipment and operation of flag ships to comply with minimum safety requirements.
The remaining four sources discuss SOLAS and other SAR conventions only in brief. Sharp and colleagues [14] state that the German naval vessels were required to conduct migrant rescue missions when SOLAS maritime law applied. When SOLAS actions were carried out, a medical response appropriate to mass casualty medical management was often required. Similarly, Hillman and colleagues [13] state that SOLAS operations require specific supplementary medical equipment, including resources for paediatric care. Panebianco [8] references UNCLOS and article 78.3 of the Treaty of Lisbon which “opens the way for such solidarity measures to be taken among member states in emergency situations” (p. 13). Finally, Patalano [18] highlights that the legal obligation to rescue those in distress at sea originates in a longstanding sense of duty to the community amongst seafarers.
3.4 Security, humanitarianism, and operational differences
Several naval and military operations involved in providing maritime medical care to migrants rescued at sea arise in the sources identified by this scoping study. Those discussed in the most detail are: Operation Mare Nostrum, Operation Triton, and EUNAVFOR MED (Operation Sophia). Three sources offer comparison of these operations and the motivations for them [8, 17, 18]. Patalano [18] argues that Mare Nostrum, an Italian naval operation run from October 2013 to October 2014, was the most effective response to the Mediterranean migration crisis. Mare Nostrum met core security requirements, intercepting 99% of migrants before they reached Italy, allowing for screening, identification and control of arrivals and arrest of human smugglers while also proactively preventing further loss of life at sea. Patalano [18] states that Mare Nostrum and its successor, Operation Triton, had little in common; the FRONTEX Operation Triton was run on a third of the budget, monitored a smaller area and focused predominantly on border surveillance. Panebianco [8] echoes these sentiments, arguing that Operation Triton is less effective than Mare Nostrum in managing the crisis as its primary purpose is border control and its core patrol area is too small to adequately conduct SAR missions. Finally, Llewellyn [17] discusses these differences further, critiquing both Mare Nostrum and Operation Triton and highlighting logistical differences between them. The particularities of EUNAVFOR MED are only discussed by Panebianco [8]; EUNAVFOR MED is described as the most innovative component of the EU response to the migration crisis and as closely modelled on Mare Nostrum.
The comparisons drawn between these operations are closely linked to another important theme in this body of literature; the tension between humanitarianism and security. Mare Nostrum, Triton and EUNAVFOR MED all had a significant focus on disrupting human smuggling and trafficking networks through intercepting boats in the Mediterranean [8, 17, 18]. Due to SOLAS and other international conventions, however, they are required to rescue people on these boats who are in distress at sea. As highlighted by Llewellyn [17], “the distinction between a control operation and a rescue one is not always obvious, since the boats used to transport migrants are often in poor condition” (p. 11). Within the sources included in this scoping study, Mare Nostrum and EUNAVFOR MED are presented in a humanitarian light; they are security missions but that are also proactively saving lives at sea. In contrast, Triton is presented as a security mission aimed at enforcing the EU’s external borders and combatting illegal migration. Nevertheless, FRONTEX officials have continuously couched Triton in humanitarian terms of saving lives [17]. The tension between humanitarian SAR and security interests is a highly politically salient topic and these operations have faced criticism from both sides of this debate.
3.5 Inter-stakeholder politics and collaboration
There are many stakeholders involved in the military medical response to the Mediterranean migration crisis. The sources identified in this scoping study outline examples of collaboration between these stakeholders and the politics and conflicts between them. The multi-faceted response to the Mediterranean migration crisis necessitated collaboration between many state and non-state actors. For example, EUNAVFOR MED (Operation Sophia) is a military operation conducted by 22 European states [8]. Examples of state and non-state actor collaboration are evident in the civil-military cooperation between the Italian navy, the Italian Red Cross and Save the Children; these NGOs were present on board some Mare Nostrum ships to provide relevant services, including medical care [8, 18]. Collaboration was also vital for air evacuation of rescued migrants in need of hospital care and between state and commercial vessels when commercial vessels responded to SOLAS calls [8, 14]. Importantly, Llewellyn [17] highlights that, in the Italian response, confusion of armed forces’ roles was not uncommon and that such confusion can obstruct the democratic control of actors involved in the response. According to Patalano [18], similar confusion was avoided in the case of Mare Nostrum due to the establishment of a clear chain of command.
Collaboration has not always been successful in response to irregular Mediterranean migration; in 2013 and 2014, EU countries were highly divided over the appropriate response and did not adopt an approach of collective responsibility, leaving Italy to carry out Mare Nostrum unassisted [8, 18]. Three sources reference the conflict over the ‘pull factor’ theory as a source of disagreement between countries about appropriate responses [8, 17, 18]. Local politics and public opinion also impacted the ability of stakeholders to collaborate appropriately; populist and xenophobic movements increased during the migration crisis, impacting the humanitarian response capacities of states [8].
3.6 Health of Migrants and the provision of maritime medical care
Three sources identified in this scoping study provide an in-depth discussion of the health of migrants rescued in the Mediterranean. Kulla et. al. [15] conducted a secondary analysis of medical data collected on German naval vessels of people rescued in distress at sea. Of the 2656 people rescued from ten different boats, 16.9% required medical treatment. The primary recorded diagnoses were dermatological diseases (55.4%), internal diseases (27.7%) and trauma (12.1%), however, Kulla and colleagues [15] stress that symptom patterns varied significantly between boats. Significantly more males (18.3%) required treatment than females (12.1%), while 5.6% of infants and 14.2% of children required treatment. The other sources that discuss the health and provision of care to rescued persons do not provide a statistical breakdown of the health conditions on board and the demographics of those in need of treatment. Despite this, Sharp and colleagues [14] demonstrate the vast diversity of health issues of rescued migrants through the case studies that they present, ranging from dehydration and collapse to gastritis and chest sepsis. Like Kulla et. al. [15], Sharp et. al. [14] highlight the variability of health status between boats. Both articles postulate that these differences are due to different conditions between groups before they embarked on their sea journey, for example due to distinct accommodation, travel length and personal circumstances. All sources that discuss the health of migrants highlight that some rescued women will be pregnant; Henning et. al. [12] cite the UNHCR estimate that 0.002% of rescued women will be pregnant, though 3.4% of women in Kulla and authors’ [15] sample were pregnant and the proportion of pregnant women varied greatly between Henning and authors’ case studies [12].
Due to the vast diversity of health issues of rescued migrants, rescuers must be prepared to appropriately treat many different conditions [12]. Additionally, medical personnel on board rescuing ships face the challenge of conducting urgent initial assessment and treatment of large groups of rescued persons [14, 15]. These challenges required the creation of medical teams that were tailored to the specific humanitarian setting of migrant rescue [12, 13, 14]. Bespoke medical supplies were also necessary; for example, a maternity delivery box was created for a UK vessel to support clinicians in the event of a patient in labour [14]. Measures were also taken to protect the health of ships’ crews and medical teams, including the use of personal protective equipment (PPE) and positioning of treatment areas to maximise infection control [12, 15]. Training for mental health resilience also proved an important activity, particularly to prepare for the management of mass drownings. In these events, body recovery was conducted by pre-selected volunteers out of view of other people on board [14]. Geraghty [16] displays the potential severity of these events, discussing a mass drowning of 200 to 300 people in front of a response ship.
4. DISCUSSION
This scoping review was conducted with close attention to Aksey and O’Malley’s [9] methodological framework and advancements made by Levac et. al., [10]. The search strategy identified eight sources that include a diversity of disciplines and perspectives, allowing this study to map the breadth of key issues on the topic. Five academic articles are included; one commentary, one secondary data analysis and three operational articles that benefit from the first-hand experiential knowledge of their authors. One source [16] is an abstract from conference proceedings for which there was unfortunately no full text available. The remaining two sources are from the grey literature; a working paper and an observational research report.
The authors had hoped to include additional grey literature, such as policy reports from NATO, FRONTEX, and national armed forces, however none were identified by the search strategy. Due to this, the study lacks the official perspectives of these organisations and operational details that would have benefitted the analysis. Nevertheless, the sources identified allow a valuable analysis of the legal and political context of the military medical response to the Mediterranean migration crisis, the conflicts and collaboration between important stakeholders and valuable discussion of the health and medical provisions for rescued persons. The inclusion of literature from diverse sources additionally displays tensions within this body of literature and a relative lack of overlap in important themes between the military medical literature and social science literature.
Some important gaps in the literature included in this study can be identified. For example, the full range of countries involved in this response are not covered by the study. Notably, no papers from Greece were found, despite it being a primary entry point to Europe for people crossing the Mediterranean. Additionally, while more than 20 European states contributed to Operation Sophia, the sources identified by the literature search only discuss the role of four of these countries in the maritime medical response to the crisis. This limitation could be attributable to the sole use of English language sources.
This scoping study has aimed to map relevant literature on the role of the military in the provision of maritime medical care to migrants rescued in the Mediterranean. The first important finding of this study is that all maritime medical care provided to rescued persons is situated within compliance to international legal requirements; these legal obligations are highly prominent in the literature and decision-making processes relevant to this response, eclipsing humanitarian and security concerns. The majority of sources included in the study specifically contextualised the medical responses in reference to SOLAS. SOLAS stipulates that crew members must be given instructions on first aid care for hypothermia and other appropriate procedures [19], however, further details on the provision of medical care are not clarified. The SAR convention, discussed in Llewellyn [17], defines rescue more broadly than other international conventions and includes the provision of initial medical care as a component of rescue missions [20]. It is important to note that SOLAS events are national responsibilities.
The same international law provisions apply to the variety of operations conducted in the European response to the Mediterranean migration crisis. However, as demonstrated by comparisons between operations Mare Nostrum, Triton, and EUNAVFOR MED, different approaches to rescue were taken throughout the course of the crisis. These differences were closely tied to political context and couched in terms of either security or humanitarianism depending on the context and audience. The framing of the operations and the political pressure on their conduct did not disrupt the legal requirement to rescue those in distress at sea. It did, however, impact the scope and efficiency of these rescue operations. While a comparison of the medical care provided between these operations is not possible in this article as no identified sources discussed the medical care arrangements in Operation Triton, it can be concluded that Mare Nostrum and Operation Sophia were more able to address the health needs of migrants at sea because they were more efficient at SAR. Panebianco [8] and Patalano [18] both stress that Mare Nostrum was more efficient than Operation Triton as Triton was limited by its small patrol area, focus on border security, and limited budget. This insight highlights that for operations in the Mediterranean to truly contribute to the reduction of the loss of life at sea, including through the acute medical care provided, they must have a genuine, proactive commitment to SAR activities.
The extent of civil-military cooperation discussed in the sources included in this scoping study is extremely interesting. This study demonstrates robust collaboration between military responders and NGOs including Save the Children and the Red Cross during Mare Nostrum. EUNAVFOR MED also demonstrates successful collaboration between the naval forces of European countries and their acceptance of the migration crisis as a shared responsibility. While the tensions and politics between some stakeholders, such as countries and armed forces departments were discussed, difficulties with NGOs were not. Possible difficulties in cooperation with NGOs include differences between strategic plans and goals of military and NGO actors, differences in command and organisation structures, and NGO reliance on public support, especially through media [21, 22]. Research on these topics could provide valuable insight and allow for further development of civil-military cooperation.
The health needs of migrants rescued in the Mediterranean were extremely diverse; this finding is consistent with migrants rescued by the NGO Open Arms in addition to the sources included in this scoping study [23]. As predicted by Kulla et. al. [15] and Sharp et. al. [14], this is likely due to the diversity in migration experiences and journeys before attempted crossing of the Mediterranean. Demonstrably, in a study of over 200 recently arrived migrants, McMohan and Signoa [5] found that participants had traversed 36 different countries in 68 different combinations before reaching Europe, and that 68% travelled for between 7 and 18 months. As forms of transport and pathogenic and environmental exposure during migration journeys have important implications for migrant health and safety, this diversity of experiences is likely to account for the diversity of health outcomes seen in rescued migrants [2]. Healthcare provided during SAR operations should focus on acute health issues, but migrants’ potential exposure to infectious diseases during their journeys must be considered and measures must be taken to prevent the infection of others on board. The sources in this study discussed using insights from previous operations in the Mediterranean to develop bespoke medical teams, supplies and facilities for response as part of the EUNAVFOR MED operation. Given the complexity of health needs of migrants rescued at sea, search and rescue missions must be equipped to address a variety of health conditions that would likely not be relevant to SAR missions in other contexts. This highlights the importance of having specific SAR vessels in operation in the Mediterranean as commercial vessels, obliged under international law to rescue those in distress, are unlikely to have the relevant expertise and equipment on board. Finally, it is also extremely important to acknowledge the difficulty of these rescue operations for the rescuers themselves. This is addressed in relation to body recovery and the development of resilience amongst the medical crew, but could benefit from further discussion relating to shift duration. Both body recovery and shift duration are predictors of PTSD and burnout amongst rescuers; efforts must be taken to mitigate these outcomes and promote sustainability of response [24].
In absence of safe and legal channels, irregular migration across the Mediterranean will continue. The security regimes enforcing Europe’s Mediterranean border have changed, including with the replacement of Operation Sophia with Operation Irini in early 2020 [25]. Like its predecessor, the primary objective of Operation Irini is not to rescue migrants in distress at sea; the operation is intended to implement the UN arms embargo on Libya and, secondarily, to disrupt human smuggling and trafficking activities in the Mediterranean [25]. At the time of writing, the medical arrangements on-board Operation Irini vessels are unclear, and the impact of this new operation on the involvement of military in the provision of maritime medical care to migrants is, as yet, unknown. However, in light of the contemporary Covid-19 pandemic, insight into this has gained upmost importance. Covid-19 adds considerable complexity to the requirement to rescue those in distress at sea and a host of more stringent protective measures have been recommended to protect vessel personnel [26]. Covid-19 additionally increases the importance of screening measures performed during rescue operations; by intercepting migrants at sea, appropriate biosecurity measures, such as quarantine, can be implemented, protecting host nations from potential health threats. It is essential that such biosecurity measures address health risks without preventing entry to those seeking asylum, as has already occurred in Cyprus and Malta [27].
Further research regarding the role of military in the provision of medical care in the Mediterranean is required, especially research that brings together the key themes identified in this scoping review. No articles discussed the impact of stakeholder collaboration or the tensions between security and humanitarian missions on the quality of care provided to rescued migrants. Qualitative interviews with key stakeholders could shed valuable light on these topics. While rescue operations conducted by military forces did save lives at sea, an unacceptable number of lives were lost in this crisis. Irregular migration across the Mediterranean will continue, and research is necessary to establish best practice in response to ensure migrants’ health is supported and their human rights respected.
5. CONCLUSION
This scoping study captures evidence of the military medical contribution to the response to irregular migration in the Mediterranean and adds to the academic literature on this subject. It has shown that the sovereign country’s navies involved in the EU and NATO humanitarian and border security operations were very aware of their responsibilities under SOLAS and wider international humanitarian law. There is good evidence of collaboration between the military organisations, wider civilian authorities and NGOs. The four papers by military authors demonstrate robust medical planning to meet the health needs of migrants, the potential risks of disease transmission from migrants to their rescuers, and an awareness of the psychological demands of the mission on naval personnel. Organisational learning from this experience has been adopted in NATO doctrine and in the MARCOM operational instructions.
Whilst it is too early to understand the impact of the Covid-19 pandemic on the underlying causes of migration, it adds a further degree of complexity to the medical aspects of SAR missions. Several gaps in the knowledge on this topic remain and necessitate further research. It would be helpful to have a fuller picture of the contribution of all of the navies involved in this response, especially those of Italy and Greece. It would also be worthwhile to explore the cultural differences between military, civilian and NGO organisations and medical personnel and how these differences influenced collaboration between them. This is of particular importance given the need for collaboration between these actors in the wider humanitarian response to the Covid-19 pandemic.
FUNDING STATEMENT
MB is partially funded through the UK Research and Innovation GCRF Research for Health in Conflict: developing capability, partnerships and research in the Middle and Near East programme (R4HC-MENA) ES/P010962/1.
SE was funded by the King’s Undergraduate Research Fellowship programme to undertake this research. The funding sources had no involvement in the design, research, writing, or submission of this article.
DECLARATION OF INTEREST
FLR was the Medical Advisor to the NATO Allied Military Command until August 2020. MB and SE have no competing interests to declare.
Order of Authors:
Sonora Rose English, BA
Conflict and Health Research Group, School of Security Studies, King’s College London,
London, UK WC2R 2LS
Martin CM Bricknell, PhD, DM, MMedSci, MBA, MA
Conflict and Health Research Group, School of Security Studies, King’s College London,
London, UK WC2R 2LS
Filippo La Rosa, PhD
Head Medical Division (NMED Acos), Special Advisors Group – Support Directorate,
Allied Maritime Command, Atlantic Building, Northwood Headquarters, Sandy Lane,
Northwood, Middlesex, UK HA6 3HP
6. REFERENCES:
1. M. McAuliffe et. al., World Migration Report 2020, IOM, Geneva, 2020. https://publications.iom.int/system/files/pdf/wmr_2020.pdf (accessed 27 August 2020).
2. I. Abubakar, R.W. Aldridge, D. Devakumar et. al., UCL–Lancet Commission on Migration and Health, The Lancet 392 (2018) 2606-2654. http://dx.doi.org/10.1016/ S0140-6736(18)32114-7.
3. [dataset] IOM, Mixed Migration Flows in the Mediterranean and Beyond, Flow Monitoring Compilation, 2015 Annual Report. https://www.iom.int/sites/default/files/situation_reports/file/Mixed-Flows-Mediterranean-and-Beyond-Compilation-Overview-2015.pdf (accessed 27 August 2020).
4. UNHCR, Refugee and Migrant Sea Arrivals in Europe, Monthly Data Update: June 2016. https://data2.unhcr.org/en/documents/download/49921
5. S. McMohan, N. Sigona, Navigating the Central Mediterranean in a Time of “Crisis”: Disentangling Migration Governance and Migrant Journeys, Sociology 52:3 (2018) 497-514. https://doi.org/10.1177/0038038518762082
6. P. Fargues, Four Decades of Cross-Mediterranean Undocumented Migration to Europe: A Review of the Evidence, IOM, Geneva, 2017. https://publications.iom.int/system/files/pdf/four_decades_of_cross_mediterranean.pdf (accessed
27 August 2020).
7. S. Panebianco, The Mediterranean migration crisis: border control versus humanitarian approaches, Global Affairs 2:4 (2016) 441-445. https://doi.org/10.1080/23340460.2016.1278091
8. S. Panebianco, The Mare Nostrum Operation and the SAR Approach: the Italian Response to Address the Mediterranean Migration Crisis, EUMedEA Online Working Paper Series, 3 (2016).
http://www.dsps.unict.it/sites/default/files/files/panbianco_EUMedEA_JMWP_03_2016__.pdf
(accessed 27 August 2020).
9. H. Arksey, L. O’Malley, Scoping Studies: towards a Methodological Framework, Int. J. of Soc. Res. Methodol. 8:1 (2005) 19-32. https://doi.org/10.1080/1364557032000119616
10. D. Levac, H. Colquhoun, K.K. O’Brien, Scoping Studies: Advancing the Methodology, Implementation Sci 5 (2010). https://doi.org/10.1080/1364557032000119616
11. D. Moher, A. Liberati, J. Tetzlaff, D.G. Altman, The PRISMA Group, 2009. Preferred Reporting Items for Systematic Reviews and MetaAnalyses: The PRISMA Statement. PLoS Med. 6:7,
e1000097. https://doi.org/10.1371/journal.pmed.1000097
12. D.W.C. Henning, A. Bennett, Role 1 Enhanced: a new paradigm in humanitarian operations. J.
R. Nav. Med. Serv. 103:1 (2017) 32-34. https://jrnms.com/JournalArticle.ashx?ID=12385 (accessed 27 August 2020)
13. C.M. Hillman, R. Horrobin, S. Mills, S. Mercer, Consideration of the Medical Care and Biomedical Support of Women and Children on Role 2 Afloat Maritime Contingency Operations J. R. Nav. Med. Serv. 103:1 (2017) 21-25. https://jrnms.com/JournalArticle.ashx?ID=12382 (accessed 27 August 2020).
14. W.M.J. Sharp, W.J. Tanzer, B. Castledine, Operation LITTEN: a Year Delivering Medical Care during the Peak of the Mediterranean Migrant Crisis, 2016-2017, J. R. Nav. Med. Serv.105:2
(2019) 80-88. https://liveicomgrshot.blob.core.windows.net/jrnmsfiles/articles/423_jrnms-105-80.pdf (accessed 27 August 2020).
15. M. Kulla, F. Josse, M. Stierholz, et al. Initial assessment and treatment of refugees in the Mediterranean Sea (a secondary data analysis concerning the initial assessment and treatment of 2656 refugees rescued from distress at sea in support of the EUNAVFOR MED relief mission of the EU), Scand. J. Trauma. Resusc. Emerg. Med. 24 (2016). https://doi.org/10.1186/s13049-016-0270-z
16. A. Geraghty, 1706b Naval Service Operations in the Mediterranean: a Medical Battlefield?, Occup. Environ. Med., 75 (2018). https://doi.org/10.1136/oemed-2018-icohabstracts.1070.
17. S. Llewellyn, Search and Rescue in Central Mediterranean Sea. http://www.migreurop.org/IMG/pdf/report_wtm_migreurop-arci-ep_08242015.pdf , 2015
(accessed 27 August 2020).
18. A. Patalano, Nightmare Nostrum? Not Quite, The RUSI J. 160:3 (2015) 14–19. https://doi.org/10.1080/03071847.2015.1061253
19. Lloyds Register, SOLAS: International Convention for the Safety of Life at Sea (2009) www.mar.ist.utl.pt/mventura/Projecto-Navios-I/IMO-Conventions%20(copies)/SOLAS.pdf
(accessed 27 August 2020)
20. R.L. Kilpatrick Jr., A. Smith, The International Legal Obligation to Rescue during Mass Migration at Sea: Navigating the Sovereign and Commercial Dimensions of a Mediterranean Crisis, Univ. of San Fran. Marit. Law J. 28:2 (2015) 141-194 https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3508389 (accessed 27 August 2020)
21. NATO, AJMedP-6 Allied Joint Civil-Military Medical Interface Doctrine, NATO Allied Medical Publication, NSO, 2015.
22. NATO, ATP-03.4.1.2: Multinational Maritime Support of Humanitarian Operations, NATO Allied Tactical Publication, NSO, 2015.
23. G. Cañardo, J. Galvez, J. Jimenez et. al., Health Status of Rescued People by the NGO Open Arms in Response to the Refugee Crisis in the Mediterranean Sea, Conflict and Health 14 (2020). https://doi.org/10.1186/s13031-020-00275-z
24. V.E. Chatzea, D. Sifaki-Pistola, S.A. Vlachaki et al., PTSD, Burnout and Well-Being among Rescue Workers: Seeking to Understand the Impact of the European Refugee Crisis on Rescuers, Psychiatry Res. 262 (2018) 446–451. https://doi.org/10.1016/j.psychres.2017.09.022
25. A. Metelko-Zgombic, COUNCIL DECISION (CFSP) 2020/472 of 31 March 2020 on a European Union military operation in the Mediterranean (EUNAVFOR MED IRINI), Official J. of the E.U. (2020). https://www.operationirini.eu/wp-content/uploads/2020/04/200401-CDIRINI-in-OJ.pdf (accessed 27 August 2020).
26. MARCOM, COVID-19 – Revision 7 MARCOM Guidance on Information Prevention and Reporting, NATO, Northwood, 2020.
27. O.S. Diez, A. Neidhardt, M. De Somer, et. al., Policy Update May 2020, European Policy Centre, 2020. https://www.epim.info/wp-content/uploads/2020/05/EPIM-Policy-Update-May-2020.pdf
(accessed 27 August 2020).
Date: 05/20/2021


