Article: Rolf von Uslar
The Multinational Medical Coordination Centre – Europe (MMCC-E) and New Realities in Security and Defence Policy
Introduction
The security situation in recent months has become even more challenging than it developed in 2014 and 2022. Europe must assume full responsibility for its defence in order to maintain peace in freedom through deterrence. Calls for a new turning point in German security and defence policy are justified. In addition to national efforts, efficient military cooperation between European nations is necessary. This includes effective medical support. As early as 2018, the Multinational Medical Coordination Centre-Europe (MMCC-E) was established at the initiative of Germany in response to growing calls for a multinational military health system. It provides medical coordination, planning and advice to European nations, NATO and the European Union.
MMCC-E plays a key role especially in the context of the current medical action plan of the Committee of the Chiefs of Military Medical Services in NATO (COMEDS). Using operational design, MMCC-E plans and directs its activities for the EU and NATO.
The flagship for assessing and enhancing multinational medical cooperation is the Casualty Move (CAMO) exercise series. This year’s CAMO25 will be the largest military exercise in Germany in terms of the number of nations involved.
Background and establishment of the Multinational Medical Coordination Centre-Europe
After Russia’s invasion of Ukraine in 2014, NATO strategy was adapted to new risks. Member States made corresponding changes to their national policy documents. The focus of German Armed Forces is thus no longer on international crisis management, as was the case in the past 25 years, but on national and collective defence. Multinationality in Europe gained further importance with this shift in focus toward national and collective defence, because many European nations can provide individual high-quality medical elements but not a complete continuum of care. With the Framework Nations Concept (FNC) of 2015, Germany introduced the idea of pooling and coordinating the elements of various nations in capability clusters, each led by a framework nation. From the start, Germany has been the framework nation for medical support, among other things. The Medical Support FNC cluster developed the idea of conducting this important work as a full-time task in a small but effective team.

Figure 1: MMCC-E nations in blue Source: MMCC-E
Initially referred to as MMCC/EMC, MMCC-E is based on the declaration of intent of initially 10 nations, an EU project of PErmanent Structured COoperation – the PESCO Project “European Medical Command” (EMC) – with German structural support from a national project to reverse personnel trends. Today, MMCC-E has 19 active member countries and five nations in an observer role (Figure 1). Switzerland was welcomed as a participating nation in March 2025. Finland has also submitted a request for full membership.
MMCC-E is based in Koblenz and is a division of the Bundeswehr Medical Support . It is composed of staff from seven countries: Belgium, France, Hungary, Luxembourg, the Netherlands, Slovakia, and Germany. A staff officer from Poland is expected in the second half of 2025.
MMCC-E has the following tasks:
1. supporting multinational medical coordination efforts,
2. improving the readiness of medical C3 (command, control, consultation) and preparedness,
3. improving medical civil-military interaction and
4. coordinating medical capability enhancement.
MMCC-E is therefore seen as a driver of efficiency between the medical services in Europe. For this reason, the task of coordination has priority – and is found in its very name. As it is a low-threshold exchange platform, MMCC-E represents significant added value for nations.
The functionality of medical services on operations depends in particular on (multinational) command and control capability. This is typically a weak point for all military medical services, not least because a link to civilian service providers must also be established. This aspect of civil-military communication is addressed in NATO by the term “consultation”. The traditional acronym C2 (command & control) thus becomes C3 (or MedC3 here). MMCC-E is thus particularly concerned with MedC3 issues and attempts to enhance existing command and control concepts and to increase competence through exercises.
The interlinking of civilian and military capabilities is a crucial issue for armed forces in times of peace, conflict and war. This is especially true for military medical services. Medical civil-military interaction is already a highly complex field at the national level. As Germany is a hub for military activities of all NATO members, a multinational component has also been added. Here too, MMCC-E is a much sought-after platform that provides insight into and information on the functions and points of contact of healthcare systems in Europe.
With almost every European nation describing, developing and equipping its own capabilities – which then must be laboriously reassembled to ensure interoperability – Europe faces a challenge. This is the case with the modular approach of the Alliance, which attempts to combine individual modules from different nations into functioning medical treatment facilities. A better approach is to develop capabilities together. To this end, MMCC-E conducts workshops in order to improve the understanding of needs and opportunities and to harmonise concepts on a multinational basis. A long-term goal is to harmonise procurement as well.
Medical Action Plan
Against the backdrop of the Russian invasion of Ukraine, NATO developed the COMEDS Medical Action Plan in 2024. This was the Alliance’s response to the vulnerabilities identified in the Medical Manifesto. The Medical Action Plan has been endorsed by NATO’s Military Committee and addresses the following strategic action items:
- regulatory framework and legislation,
- workforce shortages,
- mass casualty planning,
- patient evacuation, and
- medical logistics.
The first field of action, regulatory framework and legislation, refers to possible cross-border regulations which will facilitate and not impede cooperation. This includes medical credentialing, a process that verifies the qualifications of healthcare workers. Unfortunately, EU harmonisation has a long way to go, especially when it comes to non-licensed occupations.
Workforce shortages are a problem for all military medical services in NATO and the EU even in peacetime. In times of crisis or war, it is all the more challenging to have the necessary skillsets ready and in the required quantities. One possible solution to this problem is to increasingly qualify non-medical personnel in secondary medical roles in order to relieve core specialist personnel. A well-known example of this is the sideline activity entrusted to military musicians as support staff in the Medical Service of the Bundeswehr in Germany. In any event, increased training is the key to mitigating existing shortfalls of skilled personnel.
Mass casualty planning deals with preparation and especially planning in healthcare systems for the expected large numbers of patients in a war on the eastern flank of NATO/EU. Military as well as civilian service providers – not only hospitals – must take steps to maintain resilience in times of crisis and war. Such planning must be reflected in military expectations and operational plans (e.g. the German OPLAN DEU) and must be coordinated between civilian and military agencies.
Patient evacuation focuses on patient movement in war. Questions regarding the means, organisation and management of transportation must be clarified. This area too concerns both military and civilian capabilities. These tasks are multinational as they cannot be conducted effectively at the national level in collective defence scenarios (unlike in international crisis management operations).
The final strategic action item, medical logistics, is a topic that used to be a purely national responsibility from a NATO point of view. However, it is now clear that medical material logistics also must become multinational, given the existing interconnectedness of multinational capabilities. The magnitude of this task becomes clear when we consider that one category A patient consumes approximately 100 kg of individually provided medical consumables and supplies during the entire continuum of care.
Operational Design of the MMCC-E for the EU and NATO
The question now is how this Medical Action Plan can be used as a basis for planning the activities of MMCC-E? Well, the answer is simple: using the operational design tool!
Operational design (OpsDesign) is a NATO standard from the Comprehensive Operational Planning Directive, the handbook for operational and strategic planning. The objective of OpsDesign is to illustrate abstract and complex operational plans. It begins at the desired end state, which is broken down into individual objectives that in turn are addressed by lines of effort. In essence, this reflects Clausewitz’s ideas of purpose, aims and means.
The desired end state in our MMCC-E OpsDesign (Figure 2) is defined as an efficient, functional multinational medical service in all (conceivable) operations. In the first strategic field of the Medical Action Plan (regulatory framework and legislation), MMCC-E could possibly contribute by providing a situational picture of the countries. However, this is not the focus of attention at the moment. We have reformulated the second strategic field (workforce shortages) and included Trained Workforce as an objective in the OpsDesign. MMCC-E can and will contribute to this permanently. The strategic fields of mass casualty planning, patient evacuation and medical logistics can be directly addressed by MMCC-E as the objective Mass Casualty Planning, Functional Patient Evacuation and Functional Medical Logistics. We have also described the objectives Functional MedC3 and Functional (Medical) Capabilities, which we believe are missing from the Medical Action Plan. Outside the framework of the Medical Action Plan, an objective has also been formulated that is specific to MMCC-E: Formally Accepted, High-Performance Entity.
These objectives are now being addressed by lines of effort. The objective “Functional Patient Evacuation” is addressed by three lines of effort:
1. the work of MMCC-E on conceptual NATO documents for patient flow management;
2. in-house preparations for the provision of a Rearward Medevac Patient Evacuation Coordination Centre (RM PECC); and
3. the thematic development of the area Bulk Patient Evacuation.
When it comes to conceptual documents on patient flow management, we now have the Patient Flow Management Guideline (PFMG) of Allied Command Operations (ACO) as well as a draft Patient Flow Management Concept (PFMC) from Allied Command Transformation (ACT). As part of the CAMO exercise series, MMCC-E helped develop and further refine the basic ideas. In addition, MMCC-E also supports the (further) development of NATO software for patient management. All in all, these activities are also a contribution to the objective Functional MedC3.
Part of the planning for the management of patient transfer from the eastern flank is the RM PECC (see above), which is deployed at the level of the three Joint Force Commands (JFCs): BRUNSSUM, NAPLES and NORFOLK. From here, patients are distributed to national hubs (Figure 3). Remarkably, no structural and personnel preparations have been made within NATO structures for the RM PECC capability. For this reason, MMCC-E is preparing for at least one JFC (focusing on BRUNSSUM) in the event of a very short-term NATO mission in a collective defence scenario. During NATO exercises in the STEADFAST DUEL series, MMCC-E has already demonstrated this capability.
The topic of bulk patient evacuation requires extensive work, as there is currently only limited capacity available for the evacuation of large numbers of patients. We estimate that the casualty rate per brigade is 4% per day of combat. Approximately 75% of these casualties are likely to be wounded in action (WIA). In a large-scale combat operation with many major units deployed on the eastern flank of NATO, the number of patients to be evacuated could easily exceed the thousand mark. In order to be able to respond flexibly to operational situations, a mix of capabilities is required for bulk patient evacuation. Airborne patient evacuation assets, which are already available to a limited extent, must be flanked by large-capacity rail and road evacuation assets, as well as by associated maritime evacuation assets. To this end, MMCC-E was asked by Allied Command Operations to develop multinational documents through workshops so that such capabilities can also be acquired with the help of NATO common funding. For this purpose, we are using the findings of our workshop last year on rail patient evacuation.

Figure 2: Lines of effort in MMCC-E OpsDesign Source: MMCC-E
With the line of effort Civil-Military (CivMil) Coordination, MMCC-E contributes to the objective Mass Casualty Planning. For example, it cooperates with the Joint Health Group of NATO, which consists of representatives from the various ministries of health of NATO Member States. In addition, MMCC-E uses the knowledge and understanding of Member States to perform fundamental work on military and, more importantly, civilian healthcare systems. For example, MMCC-E has compiled a data set on patient flow management in times of peace, crisis and war for all Member States. Points of contact are being added. The result will be a real handbook that provides an overview that has not been available within NATO and the EU until now.
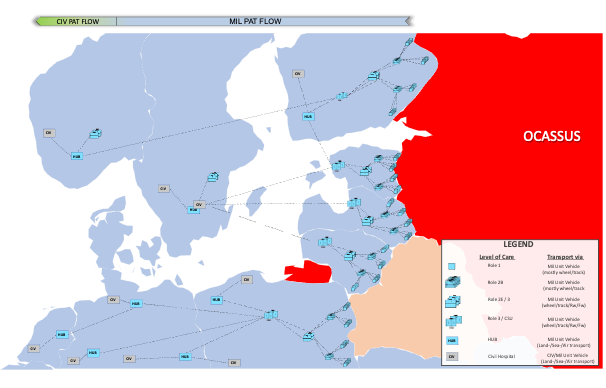
Figure 3: Patient flow from the eastern flank Source: MMCC-E
The line of effort Medical Logistics is aimed at the objective Functional Medical Logistics. It brings together all measures for developing understanding, procedures and cooperation in the field of multinational medical material logistics. MMCC-E works closely with the NATO Medical Materiel and Military Pharmacy (MMMP) Panel and has developed a tool called Paracelsus to discuss the challenges of multinational medical logistics and to develop and test solutions. MMCC-E will thus contribute to the (further) development of NATO basic documents, such as a guideline, concept and subsequent directive for medical logistics.
Exercises, especially wargames, have traditionally represented an important part of MMCC-E. They are pooled in the line of effort Exercises & Wargaming and will improve the achievement of the objective Trained Workforce. For example, MMCC-E supports the Bundeswehr Medical Academy and the Bundeswehr Command and Staff College as well as the Bundeswehr Operational Medical Support Command. It also contributes to training and exercises for many other nations. MMCC-E conducted patient flow management workshops for Estonia and Norway and casualty rate estimation (CRE) workshops for the Netherlands and Norway. The support provided by MMCC-E in the NATO Advanced Medical Staff Officer Course (better known by the acronym NAMSOC) at the Estonian Military Academy in Tartu has already become a tradition.
With the line of effort Capability Development, MMCC-E contributes to functional medical capabilities in Europe. In this context, the Substantial NATO-Georgia Package (SNGP) should be mentioned. A request from Georgia to NATO for military medical support was forwarded to Germany, which as a Framework Nation, entrusted this task to MMCC-E. The Georgian military medical service was advised and trained in operating a Role 2 medical treatment facility which had been purchased with EU funds. Multinational workshops are also an important tool in this line of effort. After such a workshop on Role 2 high-mobility medical treatment facilities, a fundamental paper was produced. A similar paper is planned for Role 1 this year. A multinational civil-military workshop in March of this year investigated the use of drones for medical services on the battlefield of the future. Here too, the results will be made available in a publication.
The two lines of effort MMCC-E’s Competences and MMCC-E’s Framework address contributions in the area of MMCC-E training and the creation of a formal framework for the objective Formally Accepted, High-Performance Entity. MMCC-E training is crucial in order to maintain and enhance existing knowledge despite changes in personnel. In our opinion, the current situation is good. It is no exaggeration to say that MMCC-E can be proud of its competence in wargaming, medical planning and CRE. Regular requests for subject matter experts prove this. The formal framework of MMCC-E has been improved in recent months by an official guest status at COMEDS. A technical agreement and a document on the support of the NATO Command Structure are still required.
The full operational design (Figure 4) includes decisive points in the lines of effort, as well as interconnections between these points. Decisive points represent specific measures or results that are particularly important to the lines of effort. The picture is complex, but it shows that many of the lines converge at CAMO25 (see the detailed article on page 48). This is therefore a central element of our work and a focus of MMCC-E.

Figure 4: Full operational design of MMCC-E Source: MMCC-E
Conclusion and Take Aways
MMCC-E has established itself as a key institution for medical multinationality within NATO and the EU. Through its active role in the implementation of the COMEDS Medical Action Plan, it contributes significantly to the resilience, interoperability and operational readiness of medical forces. It strengthens multinational medical capabilities in Europe through comprehensive workshops and their systematic documentation as well as through wargames and exercises, not only but especially in the CAMO series.In view of the changing threat situations – from possible armed conflicts to pandemics – the importance of multinational medical cooperation will continue to increase. MMCC-E will play a key role in this development as a central coordinator and innovator.
Author: MMCC-EBrigadier General (DEU MS) (OF-6) Dr. Rolf von Uslar, DD, MA
Director
Andernacher Strasse 100
56070 Koblenz, Germany
E-mail: [email protected]
Figure 1: MMCC-E nations in blue
Figure 3: Patient flow from the eastern flank
Figure 2: Lines of effort in MMCC-E OpsDesign
Figure 4: Full operational design of MMCC-E
Source for the figures: MMCC-E
Date: 06/16/2025
Source: EMMS Magazine 2025


