Article
From Hero to Pro - Change in attitude towards mental illness in deployed soldiers using the preventive computer program CHARLY
From the German Armed Forces Hospital Berlin¹ (Commanding Officer Navy Captain (MC) Dr. Knut Reuter) and from the Joint Support Office Bonn² (Commanding Officer Major General Werner Weisenburger)
Ulrich Wesemann¹, Jens T. Kowalski², Peter L. Zimmermann¹, Heinrich Rau¹, Patric Muschner¹, Sebastian Lorenz¹, Kai Köhler¹ und Gerd-Dieter Willmund¹
WMM, Volume 60 (Issue 1/2016: P. 2-7)
Scientific article
Summary
Background: German Armed Forces personnel show a high rate of combat and deployment related psychiatric disorders, first among them posttraumatic stress disorders (PTSD). To address this, CHARLY was developed as an interactive preventive platform aiming at improving resilience. The goal of this study was to show CHARLY’s supremacy in both retentive learning and attitude change as compared to traditional pre-deployment training.
Methods: To evaluate this we examined N = 35 combat soldiers deployed to Afghanistan, before and six months after deployment. Soldiers were randomly assigned to either the “CHARLY” group or the “traditional” training group. Using a knowledge quiz on PTSD and an attitude assessment on mental illness we tested for group-differences, six months after deployment.
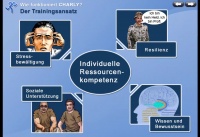 Fig. 1: Screen presentation "How works CHARLY?"
Fig. 1: Screen presentation "How works CHARLY?"
Results: Attitude toward psychiatric disorders showed significantly better values for the CHARLY group (Z = -2.13; p = .017) while knowledge showed no significant group difference. However, the total group benefited significantly from psycho-education by improving knowledge outcomes (Z = -1.67; p = .047).
Conclusions: The detected positive and stable attitude change was shown to be effected by CHARLY. As attitude change is the central prerequisite for behavior modification it could reduce the lag-period in the seeking of professional care. As the method is highly economical this finding supports the wide-spread use of CHARLY within the military deployment context.
Keywords: Prevention, attitude change, stigma, mental disorder, military deployment, predictors
Introduction
Soldiers in military deployments abroad have a high risk of experiencing specific traumatizing events and of developing a trauma-related mental disorder [1, 2]. After experiencing a traumatic event, people may not only develop posttraumatic stress disorder (PTSD), but frequently other disorders like depression, generalized anxiety, and agoraphobia [1, 3]. The burden of illness for psychiatric disorders was over 20% in deployed German soldiers [4]. Posttraumatic disorders may be predicted by peri-traumatic variables such as nature and severity of the event or prevailing psychological conditions, and by posttraumatic factors like emerging psychological symptoms, cognitions, mental coping, and social support [5].
With the high numbers and great social and economic weight of mental disorders within military systems, effective primary and secondary prevention become especially important, Unlike interventions studies [6-10], inquiries into prevention in the civilian or the military contexts have hitherto not been very convincing neither in their quality nor their quantity. One systematic review of publications aiming at preventive strategies effective prior to the occurrence of potentially damaging events found no sufficient evidence of efficacy to support any justified recommendation for elements of a preventive system of care [11]. A 2008 study on the secondary preventive efficacy of a stress management program used 40 police from Sarajevo, half of whom completed the program while the rest did not; it showed that anxiety and somatic stress reactions could be reduced significantly compared to controls [12]. In a further study on primary preventive effects, psycho-education and stress management training were used in police utilizing targeted, virtual stress exposition. At 12 months after training, participants were exposed to a simulated situational stressor equivalent to the typical police job description. Trained participants reacted in a more professional manner, with less stress, and with less of a negative attitude than controls [13].
A study by Ilniki et al. showed, in 2012, that computer-based methods and biofeedback could reduce short-term tension in traumatized people [14]. Therapeutic interventions like mental stabilization or anti-decompensation strategies, offered immediately after a traumatic event, led to reduced rates of PTSD [15].
The German Armed Forces (Bundeswehr) conducts mandatory psychological pre-deployment training for all its soldiers who are assigned a tour. This mostly takes the form of formal psycho-education classes, however of limited scope (as a rule 1 - 3 hours). As soldiers did not stop to report a need for more advanced techniques and interventions, the German Armed Forces Psychological Service commissioned a significantly more rich and structured, computer-based, interactive training platform, dubbed CHARLY (Chaos Driven Situations Management Retrieval System).
The aim of CHARLY is to strengthen the resilience, to approve the acquisition of knowledge and reduce stigma about mental disorders.
As there were no comparable data on such an approach, an evaluation of CHARLY became necessary. A number of questions had to be asked. For one, it was doubtful that a content algorithm was even able to affect knowledge and attitudes of healthy respondents. Secondly, to find out whether any such changes would also yield tangible mental health gains. This was studied in a separate inquire not covered here [16].
The aim of the present study was to examine knowledge acquisition and attitude change with regard to mental disorders, before and six months after deployment. It aimed to test whether CHARLY leads to better outcomes in these areas than traditionally taught prevention classes.
Methods
CHARLY is a preventive, interactive training platform for the improvement of resilience, psychological deployment preparation, and psycho-social support. It aims at extending one’s own coping strategies in stressful deployment scenarios in order to reduce the risk of developing a deployment-related mental disorder.
 Fig. 2: User during training: The pulse sensor (biofeedback) is applied.
Fig. 2: User during training: The pulse sensor (biofeedback) is applied.
CHARLY is used in groups of 10 to 30 participants training for one and a half days using a joint, locally networked computer array (notebook computers) so as to compare the attained results. CHARLY is comprised of three modules with a total of 12 training units. Module one consists of the unit „self-exploring“, where participants use biofeedback to learn more about their own stress reactions, and „psycho-education“, where participants are given information on stress and psychological trauma. The second module is composed of the training units „resilience as a protective stance“ and „perception of self“. Here an advisable attitude toward deployment scenarios is taught and information is given about the relationship of cognitions and emotions. Following the maxim “From hero to pro”, soldiers are given a professional view on psychological injury. The last module, in a training unit called „calming down“, centers on techniques like thought stopping, imagination, and muscle relaxation. In the unit „social support“ this module improves awareness through simulated dialogues about how to spot possible acute stress reaction.
Participants in the interactive training platform were permitted self-directed training within a blended learning environment. Moderator-led group discussions were held, before, during, and after the training. The discussions were moderated by a specially trained military psychologist. CHARLY is based on the concept of “serious gaming”. Using aliases and a point system, inter-individual comparisons are possible. This improves motivation in those modules or units where points can be gained. Participants select their own areas of concentration within the platform by their own choice.
The control group was trained formally by a psychologist, during the same time-span. It received information on development, prevention, symptoms, and management of deployment-related posttraumatic stress disorder.
Participants
The study started with N = 67 soldiers of the German Armed Forces Joint Medical Service deployed to Afghanistan a part of the International Security Assistance Force (ISAF). They served either in a field hospital company, a forward medical post, or as medics accompanying land-based combat troops. In a randomized sample they were either assigned to the intervention group (CHARLY) or a control group (CO). Randomization was done by lottery. We excluded participants who had acute psychiatric illness according to ICD-10. The drop-out rate was rather high at n = 32 , i.e., 47.8 % but was assumed to be expected in a military sample and given the extended study period [17].
Assessments were done before psychological pre-deployment training and six months after deployment. Study questionnaires were administered to participants by trained healthcare workers. At six months after their return, soldiers were mailed the same questionnaires home. The four month long ISAF contingent deployment we studied began in June, 2012.
The retained ratio at the second assessment was 52,23 % (n = 35 respondents), 19 of which were in CHARLY-group and 16 were controls. Average age of the studied soldiers was 29.77 years (SD = 5.451; range = 22 – 42). Gender distribution was 20 male and 15 female participants. 20 participants (57,1%) reported to be living in a partnership, 15 participants (42,9%) said they had no partner. Military rank structure showed 3 (8,6%) enlisted soldiers, 28 (80%) non-commissioned officers and 4 (11,4%) officers. 26 (74,3%) participants in the study were in time-limited enlistment and 9 (25,7%) were (life-long) career soldiers. As regards educational status, 3 (8,6%) of participants had finished primary or elementary school, 23 (65,7%) had obtained a middle-school diploma, 1 (2,9%) a restricted high-school diploma and 8 (22,8%) the unrestricted high-school diploma, or Abitur. Soldiers had been deployed, on average, for 2.03 times (Mdn = 1.0). Mean days of service abroad was at 273.23 (Mdn = 191.0; Range = 89 – 886).
Testing Procedures
Attitudes: To assess subjective attitudes toward psychological injury and deployment stress, the private firm ESG Elektroniksystem- und Logistik-GmbH, in 2009, had developed a questionnaire on commission by the German Armed Forces (e.g. I feel resilient, so deployment stress does not affect me). This instrument contains items on deployment stress, traumatic events, and PTSD. The questionnaire consists of 16 items with a five-point response-scale ranging from -2 = „agree completely“ to +2 „agree not at all“. Some items in the questionnaire are inverted. The more negative the scale results are (by arithmetic mean of the single items), the more realistic, un-jaded, and healthy is the attitude of the respondent in respect to psychological symptoms and disorders. The reliability (Cronbach's alpha = .62 before deployment) is still acceptable.
Knowledge about stress and PTSD: Again, the ESG company, in 2009, developed a questionnaire to assess soldiers’ depth of knowledge about the topics of posttraumatic stress disorder, stress in general, and traumatic events. This questionnaire was designed as a multiple-choice test with 15 items in order to improve analytic objectivity. Each correctly marked answer and each answer correctly left unmarked yielded one point. Maximum score was 65 points.
Statistical Analysis
Due to small sample size we used non-parametric testing. To test whether CHARLY-group or controls would show positive change we calculated for each group a one-sided Wilcoxon signed-rank test for related samples. By means of the Wilcoxon rank-sum test for independent samples we checked whether CHARLY and CO were different at six months post-deployment. All calculations were done using the IBM® program SPSS® Statistics, Version 21. Collected data on the promotion of mental health were published separately [16].
Results
Concerning knowledge there was a significant increase for the whole sample (Z = -1.67; p = .047), while CHARLY and controls showed no difference. On attitude the Wilcoxon signed-rank test for related samples showed that CHARLY-group acquired significant (Z = -1.88; p = .031) de-stigmatization during the study period, while controls (Z = -.69; p = .244) showed no positive attitude change.
By Wilcoxon rank-sum test for independent samples we showed that, at six months after deployment, CHARLY-group had significantly less (Z = 2.125; p = .017) dogmatic attitudes than controls. Table 1 shows the results of the Wilcoxon signed-rank tests for related samples at both assessments.
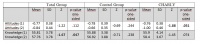 Table 1: Wilcoxon signed-rank test for paired samples to test for differences in attitudes and knowledge prior to deployment (1) and six months thereafter (2)
Table 1: Wilcoxon signed-rank test for paired samples to test for differences in attitudes and knowledge prior to deployment (1) and six months thereafter (2)
Discussion
In this study we examined the influence of the computer-based, blended-learning platform CHARLY on knowledge acquisition and attitudes toward mental disorders within a military deployment context. We published elsewhere on its effects on psychological symptoms where we found support for improved mental health in soldiers trained with CHARLY compared to controls [16].
When testing for knowledge gains, the full sample showed significant improvement in spite of the already high level (> 85 %) of previous knowledge. Separate analysis of CHARLY and controls resulted in no improvement in either. Also, at six months after deployment, there was no significant difference between CHARLY and controls. We explain the non-significant differential by the small sample size and by the originally rather high level of knowledge. Add to this, that the controls valued in-class psycho-education highly, so that it might have caused as strong an effect as CHARLY. Those training elements in CHARLY that played no substantial role with controls contribute only indirectly to knowledge gain.
With respect to attitude change, CHARLY-group did show significant differences across the study period. At six months after deployment, participants’ attitudes towards psychological symptoms and psychiatric disorders were less prone to prejudice, more health-oriented, and more realistic. The advantage of CHARLY-group over controls supports the conclusion that the CHARLY program has a more sustained effect on attitudes than traditional pre-deployment training.
The improved attitudes in CHARLY-group we detected upon follow-up can be attributed to the conveyance of advisable attitude-templates for deployment scenarios. CHARLY enhances resilience, perception of self, and the proper evaluation of cognitions and emotions, which also extends to symptoms of stress and psychopathology. CHARLY thus promises to stimulate sustainable attitude change in the pre-deployment phase which persists to beyond deployment.
This result acts as a positive counterpoint to a recent meta-analysis which resigned itself to the conclusion that currently known interventions could not effectively diminish self-stigmatization in the face of mental illness [18].
The current study is the first of its kind, using a randomized, controlled design and a structured primary prevention intervention to show positive attitude change toward psychological alterations associated with military deployments abroad. Previous studies could either detect no significant advantages from prevention [11] or had not obtained baseline data before deployment [13]. As we examined a rather small sample here, our results should be replicated in a larger sample, and also extend to other military specialties such as combat troops.
Dealing with one’s own personal health, the upcoming stresses, and one’s own competence to cope with them takes center stage with soldiers. [19]. We posit that a soldier’s attitude toward the psychological risks associated with his profession is crucial in determining the lag-period in his seeking of professional care, should he need it. Yet still, it seems that the need for research in this area remains woefully unmet [20]. It is known that soldiers with an advisable attitude seek professional help earlier and consequently reduce their risk of chronic mental illness [21].
Mobile implementation of CHARLY in-theater by the requisite staff-psychologist, while deployed, could be a means to maintain the edge and stay on top of the issue. It could improve functionally advisable attitudes and further improve resilience. Because of its low-cost equipment demands (one notebook computer suffices) and simplicity, the use of CHARLY and the associated integrative training platform could easily be integrated into the daily in-theater routine.
Limitation
The conclusive power is limited by the small sample size after accounting for drop-outs. This study should therefore be regarded as a pilot. Further research on CHARLY is forthcoming.
Core Messages
Soldiers possess a high level of PTSD-related knowledge. This knowledge is enhanced both through CHARLY and traditional pre-deployment training. CHARLY could be shown to be superior in changing attitudes on mental illness. Six months after deployment, soldiers in the CHARLY-group had significantly less prejudice about psychological symptoms and showed better health orientation than controls. This improves their seeking and accepting early professional help and thus contributes to preventing chronic disease.
Conclusions
CHARLY is an effective and economical tool for the pre-deployment training of soldiers. In a randomized, controlled study, this computer-based learning program was shown to cause a preventive effect and a less prejudicial attitude of soldiers towards mental illness. Its more comprehensive use can therefore be recommended.
References
- Kaikkonen NM & Laukkala T: International military operations and mental health - A review. Nord J Psychiatr 2015; 12: 1-6.
- Wittchen HU, Schönfeld S, Kirschbaum C, et al.: Traumatic experiences and posttraumatic stress disorder in soldiers following deployment abroad: how big is the hidden problem? Deutsches Ärzteblatt International 2012; 109 (35-36): 559-568.
- Trautmann S, Schönfeld S, Höfler M, et al.: Posttraumatic stress disorder after deployment of German soldiers: does the risk increase with deployment duration? Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013; 56 (7): 930-940
- Wittchen HU, Schönfeld S, Kirschbaum C, et al.: Rates of Mental Disorders Among German Soldiers Deployed to Afghanistan: Increased Risk of PTSD or of Mental Disorders In General? J Depress Anxiety 2013; 2:133.
- Becker-Nehring K, Witschen I & Bengel J: Schutz- und Risikofaktoren für Traumafolgestörungen. Zeitschr Klin Psychol Psychother 2012; 41 (3): 148-165.
- Rothbaum BO & Hodges LF: The use of virtual reality exposure in the treatment of anxiety disorders. Behavior Modification 1999; 23 (4): 507-525.
- Krijn M, Emmelkamp PM, Biemond R, et al.: Treatment of acrophobia in virtual reality: The role of immersion and presence. Behaviour Res Ther 2004; 42 (2): 229-239.
- Krijn M, Emmelkamp PMG, Olafsson RP, Biemond R: Virtual reality exposure therapy of anxiety disorders: a review. Clinical Psychology Review 2004b; 24 (3): 259-281.
- Baus O, Bouchard S: Moving from virtual reality exposure-based therapy to augmented reality exposure-based therapy: a review. Front Hum Neurosci 2014; 8: 112.
- Pelissolo A, Zaoui M, Aguayo G, et al.: Virtual reality exposure therapy versus cognitive behavior therapy for panic disorder with agoraphobia: A randomized comparison study. Journal of CyberTherapy & Rehabilitation 2012; 5 (1): 34-43.
- Skeffington PM, Rees CS, Kane R: The primary prevention of PTSD: a systematic review. J Trauma Dissociation. 2013; 14 (4) :404-22.
- Sijaric-Voloder S, Capin D: Application of cognitive behavior therapeutic techniques for prevention of psychological disorders in police officers. Health Med 2008; 2 (4): 288.
- Arnetz BB, Nevedal DC, Lumley MA, Backman L, Lublin A: Trauma resilience training for police: Psychophysiological and performance effects. J Police Crim Psych 2009; 24: 1-9.
- Ilnicki S, Wiederhold BK, Maciolek J, et al.: Effectiveness evaluation for short-term group pre-deployment VR computer-assisted stress inoculation training provided to Polish ISAF soldiers. Stud Health Technol Inform 2012; 181: 113-117.
- Miller L: Psychological interventions for terroristic trauma: prevention, crisis management, and clinical treatment strategies. Intl J Emerg Ment Health 2011; 13 (2): 95-120.
- Wesemann U, Kowalski JT, Jacobsen T, et al.: Evaluation of a technology-based adaptive learning and prevention program for stress response - a randomized controlled trial. Mil Med 2015 (in print)
- Wesemann U, Schura R, Kowalski JT, et al.: Context of deployment and tobacco dependence among soldiers; Gesundheitswes 2015; 77 (Epub ahead of print).
- Griffiths KM, Carron-Arthur B, Parsons A, Reid R: Effectiveness of programs for reducing the stigma associated with mental disorders. A meta-analysis of randomized controlled trials. World Psychiatr 2014; 13 (2): 161-175.
- Brenner LA, Betthauser LM, Bahraini N et al.: Soldiers returning from deployment: A qualitative study regarding exposure, coping, and reintegration. Rehabil Psychol 2015; 60 (3): 277-285.
- Hom MA, Stanley IH, Joiner TE: Evaluating factors and interventions that influence help-seeking and mental health service utilization among suicidal individuals: A review of the literature. Clin Psychol Rev 2015; 40: 28-39.
- Garcia HA, Finley EP, Ketchum N, Jakupcak M, Dassori A, Reyes SC: A survey of perceived barriers and attitudes toward mental health care among OEF/OIF veterans at VA outpatient mental health clinics. Mil Med 2014; 179 (3): 27327-8.
Pictures provided by:
Picture 1: ESG Elektroniksystem- und Logistik-GmbH
Picture 2: Frank Eggen, Berlin
Scientific article
Manuscript data:
Manuscript received on 7 October 2015, revised version accepted on 2015/12/17
Citation:
Wesemann U, Kowalski J, Zimmermann P, Rau H, Muschner P1, Lorenz S1, Köhler K, Willmund D: From Hero to Pro - Change in attitude towards mental illness in deployed soldiers using the preventive computer program CHARLY. Wehrmedizinische Monatsschrift 2016; 60(1):2-7.
A German version of this article you will find here.
Eine Deutsche Version finden Sie hier.
Date: 01/20/2016
Source: Wehrmedizinische Monatsschrift 2016/1


