Article
Implantation of endo-exo prostheses in cases of lower limb amputation – an alternative treatment option for injured soldiers? – update and case report
From the Department of Plastic, Hand and Reconstructive Surgery1 (headed by H. H. Aschoff, MD) at Sana Hospital, Lübeck (medical director: M. T. Bahr, MD), the Department of Trauma Surgery and Orthopaedics2 (headed by Colonel (MC) Prof. C. Willy, MD), and the Research and Treatment Centre for Septic Defects at the Bundeswehr Hospital Berlin (headed by Commodore (MC) K. Reuter, MD)
Summary
Introduction: Of the ore than 50,000 soldiers injured in Iraq and Afghanistan, about 2,000 required single or multiple amputations. Conventional medical care involving socket suspension prostheses may be difficult or unfeasible for some patients, depending on the length of the residual stump and the condition of the soft tissue. This case report illustrates an alternative approach that involves an osseointegrated, transcutaneous implant connected to a prosthesis.
Case report: A 35-year-old male had suffered polytrauma including traumatic transfemoral (right) and transtibial (left) amputation 12 months previously. In April 2016, the intraosseal components of the endo-exo prostheses were implanted on both sides. The use of a classic socket suspension prosthesis had failed due to soft tissue problems. In July 2016, stomata were completed and the transcutaneous exo-portions were implanted and, two days after surgery, the external prostheses were connected. As a result, the patient can stand and walk without crutches.
Discussion: Despite a high degree of perfection of conventional socket prostheses, problems with the connection between stump and prosthesis remain, primarily due to volume changes of the stump, skin irritations from sweating and mycotic infections, as well as mechanical strain, especially if the residual stump is short. Up to 72% of patients are limited in their daily private and professional lives as a result of problems with their prosthesis. About 18 % of younger patients are unable to use their prosthesis daily due to stump problems, and 51 % suffer pain on a regular basis.
Osseointegrated, transcutaneous implants with a distal connection to prostheses (endo-exo prosthesis) have been fitted for more than 100 patients at Sana Hospital Lübeck (Germany) since 1999 and allow for prosthetic treatment in otherwise untreatable cases. Patient satisfaction is high and osteoperception allows for better postural control. Although bacterial contamination of the stoma area is common, no soft tissue or bone infections developed. Amputations as a result of artery occlusive disease and diabetic microangiopathy are contraindications for treatment with endo-exo prosthetics.
Conclusion and Way Ahead: With a service life of more than 12 years, endo-exo prostheses have proven to be suitable for the treatment of amputees with stump problems. It offers soldiers who underwent amputation as a result of injury on deployment an alternative to improve their rehabilitation and professional reintegration. Hannover Medical School and the Bundeswehr Hospitals in Berlin and Hamburg, with support from Dr Aschoff, will be established as competence centres to apply and scientifically monitor this procedure.
Key words: traumatic amputation, stump care, osseointegration, endo-exo-prosthesis, osseoperception, rehabilitation, reintegration
Introduction
To date, over 50,000 soldiers have been injured during military interventions in Afghanistan and Iraq. As a result of these conflicts, the number of single or multiple amputees is assumed to be around 2,000 [1,2]. We can assume a total amputation rate of 3.3% among injured personnel and, depending on the cause of injury and the type of warfare, a rate of bilateral amputation of the lower extremities of up to 2.8% [1,3]. At times, up to 14 out of every 100 injured personnel admitted for treatment had to undergo an amputation – in particular during the time period between early 2010 and mid-2011 [4]. Most amputations were transtibial (~40%) or transfemoral (~35%) [4]. About 30% of all amputees sustained multiple amputations – a marked increase over previous military conflicts [4]. In about 10% of cases secondary amputations were performed more than 90 days after the initial injury [4].
Rehabilitation after transtibial or transfemoral amputation with a conventional socket prosthesis can be difficult or even impossible, depending on the quality of the stump. A short residual femur or tibia as well as insufficient soft tissue coverage of the bone particularly limit the quality of care that a prosthetist can provide. A prosthetic fitting that does not merely connect the prosthesis to the stump with the help of a socket and liner but instead relies on an implant that is firmly integrated in the medullary space of the amputated long bone represents an entirely different treatment approach. Such a transcutaneous osseointegrated implant to connect the exo-prosthesis to is an alternative treatment option. Even patients whose mobility has been severely limited for a long time can learn to walk again, rather than having to rely on a wheelchair for the rest of their lives.
Using a case report as an example, this article describes and discusses the possibilities of endo-exo prostheses and their potential relevance for the treatment and rehabilitation of soldiers injured in accidents or on deployment.
Case report
Medical History
A then 34-year-old man was involved in a car accident in the United Arab Emirates in January 2015 and suffered polytrauma with extensive soft tissue trauma and fractures of the right femur and the left lower le g, a complex pelvis fracture, a ruptured spleen and craniocerebral trauma with subdural haematoma and an injury of the right eye (figure 1).
Figure 1: State of lower extremities after the accident. Left image: Tourniquet on the right thigh, comminution of the entire lower leg and distal thigh; Right image: Avulsion and comminution of the left lower leg with torsion of the distal portion by approx. 180°

.
Emergency surgical treatment at a local hospital included transfemoral amputation of the right leg and transtibial amputation of the left leg as well as a splenectomy. After being hospitalised in the local intensive care unit for a month, the patient was repatriated to Germany for rehabilitation.
In February 2015, a complex pelvis fracture with fracture of the lateral mass of the sacrum and a bilateral fracture of the inferior pubic rami were diagnosed in the rehabilitation facility and the patient was transferred to a nearby trauma centre. After conservative consolidation of the pelvis fracture and surgical revision of the stump of the right thigh with refixation of a shell-like bone fragment to the distal end of the femur to prevent a pointed bony stump, rehabilitation therapy began in April with the patient being fitted with socket prostheses on both sides. He returned home in April 2015 and was re-admitted to the trauma centre in August 2015 for further rehabilitation as planned. There, further revision surgeries on the stumps of the upper and the lower leg were once more required so that discernible progress in being able to walk failed to materialise for the patient (Figure 2). The medical report from his first in-patient treatment in Lübeck includes no further details on this, but the patient himself described his great personal dissatisfaction with the process thus far. Having learnt about the option of transcutaneous osseointegration, he presented of his own accord at Sana Hospital in Lübeck for endo-exo consultation in January 2016.

Figure 2: Patient at the time of presentation in January 2016; Mobility limited to wheelchair; walking or standing with the fitted socket prostheses impossible because of insufficient fitting of the socket as a result of constantly changing volume of the stumps, which was associated with intense pain.
Initial Clinical Findings
Clinical examination showed a 35-year-old patient in a good general state of health with no serious comorbidities that would have constituted a contraindication when it comes to endo-exo prosthetics. The state of the soft tissue on both extremities also showed no restrictions with regard to the procedure.
Diagnosis
X-rays of the residual femur show a slightly dehiscent bone lamella at the distal end of the bone with an otherwise normal remaining long bone. At 115 mm, the tibia stump was long enough to attach a custom-made implant. A CAT scan of the pelvis showed full osseous consolidation of the fractures of the sacrum. Only the fracture of the left inferior pubic ramus showed signs of pseudoarthrosis, which did not, however, constitute a contraindication with regard to the planned implantation (figure 4).
Figure 4: X-rays with planned implants sketched in.

Therapy and Course
After the bespoke manufacture of the implants, the so-called endo-modules were implanted in the right femur and left tibia stump in the first surgical procedure in April 2016. The femur stump was shortened by 5.5 cm and the dehiscent bone lamella was removed. Post-operative recovery was complicated by pneumonia and temporary anaemia due to blood loss. Increased bleeding from the Redon's suction drains in the right thigh stump required revision and evacuation of haematoma the evening of the day of surgery.
Following three days of intensive medical care, the patient recovered quickly, the wound healed per primam, and post-operative X-ray showed the implant to be positioned as intended (figure 6a). The patient was already experiencing chronic pain when he was admitted to hospital, which required intensive treatment by our dedicated pain therapist throughout the entire hospital stay.
At the end of April, the patient returned home. Re-admission for the second step of surgery was scheduled for mid-July 2016, at which point both stumps were "stomatised" as planned. To create a "stoma", a perforation is cut into the skin covering the bone so that the external parts of the prosthesis (exo-portion) can later be connected with the metal implants that are firmly integrated in the bone shaft (endo-portion) to form the endo-exo prosthesis.
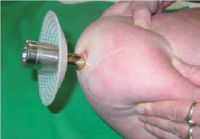
Figure 5: Stoma with transcutaneous implant to connect to the exo-prosthesis
Two days after the stomata were created, an orthopaedic technician mounted and aligned the exo-prostheses to the implants so that, for the very first time since the accident, the patient was able to feel direct contact with the ground via the implants connected to the bone that same day. Walking training began a week later in the nearby rehabilitation centre. At the time of writing (8 November 2016), the patient is pain-free and mobile with bilateral integral leg prostheses that bear his full weight; the soft tissue around the area where the implant penetrates the skin is free from irritation (figure 6b). A follow-up examination has been scheduled for February 2017.
Discussion
Conventional Prosthetic Care

Conventional prosthetic care of patients with amputations of the lower or upper leg using prostheses with sockets that envelop the stump has seen impressive improvement in recent decades. Materials as well as the manufacturing know-how of orthopaedic engineers have led to a high degree of perfection when it comes to manufacturing the connection between the amputation stump and the prosthesis. Nowadays, computer-controlled prosthetic knees, for example, allow top athletes to deliver similar or even better performances compared with healthy persons. Nevertheless, some patients experience functional limitations, which can, in summary, be attributed to improper fit of the stump and the prosthesis socket. This may be the result of fluctuations in volume of the stump due to even minor changes in the patient's weight. The skin is often chronically irritated by increased perspiration and pressure marks develop, leading to dissatisfaction with the fit of the prosthesis. These issues are particularly common in patients with short amputation stumps and unfavourable soft tissue conditions (e.g. femur < 15 cm, tibia < 8 cm).
Figure 6: X-ray (a) and clinical presentation (b) after bilateral endo-exo-prosthetic treatment, two days after the second implantation surgery (creation of a stoma)
Structured interviews of 2039 amputees carried out by researchers at the Centre for Rehabilitation Medicine of the University Medical Centre Groningen to evaluate the functioning in daily life showed that 63% (n=507) of 805 patients with conventional prostheses experienced one or more skin problems (blisters, folliculitis, sores, fungal infections) in the stump area. Such stump problems considerably impaired patients while engaging in household activities, wearing the prosthesis in the first place, or experiencing social integration and participating in sporting activities. [5] Critical evaluation of the survey results by the same working group also showed that, owing to skin problems of the stump, more than a third of these patients were indeed restricted in their use of the prosthesis and in the distances they were able to walk. [6]. A study carried out by a Dutch working group at De Vogellanden Centre for Rehabilitation in Zwolle yielded similar results and showed the rate of skin problems of the stump was more than doubled in patients with additional functional limitations of the upper extremity [7].
A study which mainly focused on trauma- and tumour-related amputations, and therefore on younger patients (n = 97), showed that only 82% were using their prostheses on a daily basis, which means that every sixth young patient was not able to use their conventional prosthesis as intended. Heat and perspiration were reported as a problem by 72% of respondents, while 62% experienced sores/skin irritation. Walking on uneven terrain was a struggle for 61% and 59% could not walk quickly. Pain in the residual limb was reported by 51%, while 47% and 46% reported structural changes leading to back pain and pain in the other leg, respectively [8].
Endo-Exo Prosthetics
For patients who experience problems with stump care, endo-exo prosthetic technology provides a treatment option that will enable them to once again attain a high degree of mobility. Rickard Branemark was the first to use this technology to treat a patient in 1990 in Gothenburg, Sweden, using a locally developed screw implant after a transfemoral amputation [9]. In Lübeck in 1999, Hans Grundei presented an implant that he had developed which was clearly different from the Swedish model in terms of surface structure and stability criteria. Beginning in 2003, Aschoff et al. further developed the technique at the Sana hospital in Lübeck [10]. While endo-exo prosthetics initially focused only on patients with transfemoral amputations, encouraging results in the following years led to an expansion of the procedure to patients with amputations of the lower leg [11]. The working groups in Sweden and Lübeck have since also gathered experience with patients after transhumeral amputations [12].
An interim evaluation of the retrospective study carried out in Lübeck on the effects of providing transfemoral amputees with endo-exo femoral prostheses showed very satisfactory results with regard to comfort, mobility and quality of life in affected patients [13, 14]. All patients considered so far reported having experienced improvements as a result of their endo-exo prosthesis; they are highly satisfied and would opt for this kind of treatment again if faced with the same decision [13, 14]. As always in prosthetics, however, achieving such positive results requires patients who are carefully selected and informed in detail as well as close cooperation between the surgeon, the manufacturer of the implant, the orthopaedic technician, rehabilitation facilities, insurance companies, and the general practitioner.
Indication/ contraindication:
Osseointegrated transcutaneous endo-exo prostheses have been clinically established and are worth being included in the treatment spectrum [10 - 14].
Endo-exo prosthetic treatment is indicated in cases where rehabilitation using a socket prosthesis has been unsatisfactory or impossible. Such cases include patients with very short amputation stumps, which can be further stabilised with endo-modules secured in place by fixation devices inserted at a right angle to the femur or tibia (femur > 10 cm, tibia > 66 mm). Severely scarred and in particular adipose stumps (e.g. thigh circumference > 60 cm) are further rewarding indications. Once the patient has been provided with all the relevant information, chronic soft tissue problems inside the socket, recurring abscesses at the rim of the socket or in the groin area as well as the patient's express interest in the procedure may constitute further indications.
So far, traffic and agricultural accidents have been the most common causes of injury that lead to patients being treated with endo-exo prosthetics. Another specific set of patients are long-time wearers of socket prostheses who, with advancing age and fading strength, increasingly experience difficulties attaching and removing their prostheses. Elderly patients are particularly interested in making the switch to osseointegrated prosthetics so as not to have to rely on outside assistance. The Lübeck hospital continues to regard as a contraindication any amputation performed as a consequence of peripheral artery disease or diabetic angiopathy.
Risk of infection and loosening of the prosthesis
Chronic bacterial contamination that does not constitute a surgically relevant pathology is common and generally results neither in deep infection of the soft tissue nor of the affected long bone. This also became evident in a study based on molecular and microbiological examinations in which 30 patients had to have the screw removed from the intramedullary base for various reasons (mostly mechanical problems). The authors were able to demonstrate that while bacterial colonisation deep in the soft tissue or on the screw thread was common (27/30), there were generally no signs of infection [15].
The clinical analysis of 119 patients treated in Lübeck thus far showed that the implant had to be removed in 13 cases (n = 5 because of deep infection, n = 6 because of soft tissue problems, n = 1 implant breakage, n=1 patient's wish). In four of those cases, the implant could be re-implanted successfully [16]. As a rule, however, osseointegrated transcutaneous endo-exo prosthetic treatment results in reliable engraftment of the bone in the three-dimensionally structured surface of the intramedullary implant and in uninterrupted service lives of transcutaneous endo-exo prosthetics of now more than 12 years in patients at Lübeck hospital.
The results so far are in line with the positive results published by the working group around R. Branemark in Gothenburg, Sweden, at Radboud University in Nijmegen, Netherlands, as well as by the working group around Muderis et al. in Sydney, Australia. None of the working groups found any surgically relevant infections around the stoma. That was the unanimous result of the discussion during the First International Symposium on Innovations in Amputation Surgery and Prosthetic Technologies in May 2016[1]. Branemark et al. described a five-year success rate of 92% and 24 months after implantation, 40 of the 45 patients (89%) reported using their prosthesis on a daily basis, compared to 57% (29 of 51) before the endo-exo implant [17]. The average score of prosthesis use improved from 47 (0 to 100) before surgery to 79 (0 to 100) two years after the coupling surgery (intramedullary implant and prosthesis; p < 0.0001). There has been a significant collective increase (p < 0.0001) of the Q-TFA[2] score (used to measure quality of life after transfemoral amputation) due to significantly improved mobility. The Short Form (36) Health Survey, a general measuring tool that is not specific to any disease and is used to evaluate health-related quality of life, showed significant general improvement in quality of life (p < 0.0001). In this patient group, the most frequent complication was superficial infection (41 instances in 28 patients). On average, every patient experienced a superficial infection every two years, which, as a rule, was effectively treatable with oral antibiotics. Three patients had to have their implant removed (n = 2 inadequate osseointegration, n = 1 deep infection). The Swedish working group observed similar results with endo-exo prostheses following transhumeral amputation [18]. The Australian working group around Muderis could also demonstrate significant postoperative improvement in 22 patients, based on the standard outcome parameters Q-TFA, SF-36, the six-minute walk test (6MWT) and the Timed Up and Go test (TUG). Muderis also describes superficial infections as the most common complication (15 episodes in n = 12), which could all be treated conservatively. He observed no severe complications. Overall, recurrent superficial infection, which can generally be treated with conservative methods, must be considered the most clinically relevant complication associated with the procedure presented in this article, while deep infection that could lead to implants needing to be replaced or aseptic loosening have thus far occurred only very rarely.
Other Advantages of Endo-Exo Prosthetics
Experience has shown that the improved tactile perception of ground contact through the bone (osseoperception) results in improved postural control, increased gait security and comfort and therefore a comparatively more favourable energy balance.
It must be noted that the exo-prosthetic portion of the endo-exo prosthesis requires that modern computer-controlled knee joints be available. In order to neutralise what could be considerable torsional force generated in a fall and to cover safety and insurance aspects of the treatment with these "high-tech" knee joints, a special rotating dual cone adapter component is available to connect the intramedullary stem to the external prosthesis. Severe fractures or implant breakage can be prevented with a custom-fit shear pin safety mechanism designed to fail when a defined torsional force develops.
Military Medical Aspects
The best possible recovery and rehabilitation as well as subsequent reintegration into service of injured personnel are not only a legal stipulation – pursuant to the Act on the Continued Employment of Personnel Injured on Operations of 18 December 2007 – but are also an indispensable obligation for ethical reasons. Without the ability to move around freely "on one's own two feet" in everyday situations, options for employment in the military are very limited. It must be noted that according to the few outcome studies available, about a sixth of all young lower-limb amputees can use their prostheses only temporarily or not at all [8]. In such cases, following individual assessment and involvement of the Bundeswehr centre of competence on issues of orthopaedic engineering, an endo-exo prosthesis can contribute considerably to the vocational re-integration of injured soldiers.
Conclusion and Way Ahead
The case presented here highlights the possibilities of osseointegrated prostheses after traumatic amputation. Over the past 17 years, the impressive merits of endo-exo prosthetics have been proven. To date, more than 100 patients have been treated with this approach. Meanwhile, implants have reached a service life of more than 12 years. Even if traffic and agricultural accidents currently represent the largest contingent of all treated patients, we can assume that particularly young, active people who have lost a limb through traumatic amputation as a result of deployment-related injury can benefit from this technology if conventional treatment causes profound problems. Therefore, patients will increasingly be recruited from military conflict areas. Innovative solutions are needed for young people with sometimes devastating multiple amputations after explosion injuries, which is also evident in the recent interest in endo-exo technology in the US. In the past year, the FDA (Food and Drug Administration) approved a Swedish implant and an implant developed in the US for clinical application of transcutaneous osseointegration with scientific monitoring. US military medical facilities have also expressed considerable interest in the promising treatment method described here. It seems that, much like the history of tooth implants, after almost two decades, transcutaneous osseointegration is now finally recognised as a valid treatment option.
We may conclude that this innovative technology, which in Germany is employed almost entirely monocentrically in Lübeck, with sparse experience in Murnau and Tübingen, will go on to help Bundeswehr soldiers with deployment-related traumatic amputation of the extremities as well as after accidents on or off duty in cases where conventional prostheses pose considerable problems.
Future scientific interest will focus on achieving desirable inert sealing of the area where the implant penetrates the skin, an optimised surface finish of the implant stem for particularly short residual bone stumps as well as the biomechanical implications of osseointegrated prosthetics.
The Trauma Department at Hannover Medical School (Director: Prof. Christian Krettek, MD) and the Department of Trauma Surgery, Orthopaedics, and Septic Reconstructive Surgery / Research and Treatment Centre for Septic Defects at the Bundeswehr Hospital Berlin (Director: Colonel (MC) Prof. Christian Willy, MD) as well as the Department of Trauma Surgery and Orthopaedics of the Bundeswehr Central Hospital in Hamburg (Director: Colonel (MC) Matthias Johann, MD) will, with the cooperation of the corresponding author, establish themselves as competence centres for endo-exo prosthetics and continue to develop the technology – including in cooperation with Murnau Hospital – and monitor it scientifically, in order to continue to optimise the rehabilitation of severely injured soldiers.
[1] The First International Symposium on Innovations in Amputation Surgery and Prosthetic Technologies was held from 12 to 13 May 2016 at Prentice Women's Hospital, 250 East Superior Street, Chicago, IL. The author has a copy of the proceedings of that meeting.
[2] Q-TFA = Questionnaire for Persons with Transfemoral Amputation
Date: 07/31/2017
Source: Wehrmedizinische Monatsschrift 2017/1


