Article: M. Lüpke
The Dental Services of the DEU Armed Foces Medical Service in the field
Maintaining the dental health of service personnel on deployment abroad is often subject to special demands and requirements. Absolute priority must be given to the preservation or restoration of unrestricted combat readiness. To ensure that the dental status of service personnel when deployed is adequate, appropriate provisions must be made at home, where the extensive oral remedial treatments they may need are available. However, even with sophisticated programs dental emergencies arising in the field cannot always be avoided.
Introduction
The dental services of the DEU armed foces are tasked with maintaining the dental health of military personnel both at home and during deployment. German combat personnel are currently participating in missions around the world – they are serving at the Horn of Africa, in Kosovo and Afghanistan. Particular problems arise in connection with ensuring that their dental health is maintained while they are in the field and absolute priority must be given to the preservation or restoration of their unrestricted combat readiness. To ensure this, appropriate provisions must be made in their homeland, where personnel can be provided with the extensive oral remedial measures they may need. However, even where such a program is in place, it is next to impossible to avoid the risk of dental emergencies arising in the field. For this reason, the appropriate infrastructure and personnel must be made available. There can be major differences with regard to actual requirements depending on the nature of the deployment – the situation in the field hospital in Mazar-e-Sharif and on board a frigate participating in Operation Atalanta are very dissimilar. One possible way of reducing the risk of emergencies arising in the field in future would be to analyse the various causes that necessitate the provision of dental treatment during deployment. With this in view, this article considers and discusses in detail the various diagnoses and treatment measures documented during the deployments of 2010.
The range of responsibilities and missions of the DEU AF have undergone major changes in recent years. Originally, an armed force raised purely for homeland defence, the DEU AF are now actively involved in military missions in many locations outside Germany. In October 2011,
 Fig. 1: current (October 2011) DEU Armed Forces missions with dental service partcipation.
Graphic: SanABw Abt. VI
Fig. 1: current (October 2011) DEU Armed Forces missions with dental service partcipation.
Graphic: SanABw Abt. VI
some 7300 personnel were participating in various missions, the majority serving with the ISAF in Afghanistan.
This, of course, means that the requirements for dental health of the personnel involved have changed. Only healthy service personnel are fully fit for duty and combat, their overall health status also being determined by their dental health. Anyone who has themselves experienced toothache can readily imagine that a soldier with pulpitis or a periodontal abscess will be in no condition to be sent on active duty. Those serving in the field are also at increased risk of wounds and injuries in the oral region, so that well trained medical personnel must be deployed together with the troops. Their skills are not only required for dental emergencies and the treatment of oral wounds and injuries; dental personnel and dental treatment facilities always represent an intrinsic element of overall medical support in the field and are integrated in the capabilities of the corresponding medical services. From the early missions of the DEU AF in Cambodia and Somalia to its current deployments in Kosovo and Afghanistan, dentistry and the related skills have always been in the forefront of medical support; and dental officers, particularly those specialised in oral surgery, have to date accompanied DEU personnel on almost all their missions.
Dental fitness classification
As a matter of course, the provision of full oral remedial measures in the homeland must take precedence. It was not without good reason that the dental fitness classification (DFC) system specified in NATO STANAG 2466 Med was adopted by the Dental Services of the DEU AF in 2006. This subsequent regulations require every serving member of the armed forces to undergo an annual dental check by a dental officer, who is then required to assess their dental status in terms of the four dental fitness classes. The dental fitness classification system makes it possible, using the results of dental examination, to predict the likelihood of a dental emergency occurring in a particular case over the following
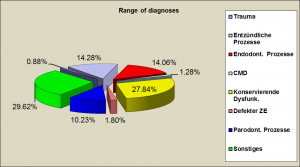 Fig. 2: Diagnoses of disorders requiring emergency treatment. Graphic: SanABw Abt. VI
Fig. 2: Diagnoses of disorders requiring emergency treatment. Graphic: SanABw Abt. VI
12 months. The definitions of the four dental fitness classes are shown in Table 1 below.
Patients with, for example, problems at a crown margin or incipient caries are categorised in dental fitness class 2. Although they will undoubtedly need dental treatment at some point, it is unlikely that they will experience a full-scale dental emergency in the coming 12 months. Patients with extensive carious lesions or dental apical disease, on the other hand, are allocated to dental fitness class 3 as it can be expected that they will need emergency treatment within that period. In this context, it should be pointed out that the vast majority of dental emergencies in the field are associated with diagnoses relating to conservative dental treatments and that this aspect is thus of particular importance. This is considered in more detail further on this article.
Only service personnel with dental fitness classes 1 or 2 are considered fit for active service. The provision of extensive oral remedial measures must thus be the primary objective of dental care in the homeland but, for various reasons, this is not always possible. However, it is essential to ensure that personnel classified as DFC 3 receive the necessary treatment so that they can be reclassified as DFC 2 at the least. Treatment of personnel with status DFC 3 thus has to receive priority.
The tasks of the Dental Service in the field
Although systematic implementation of the outlined measures will help reduce numbers of cases of dental emergencies in the field, this will not completely exclude their risk, and such an emergency may always impair the patient’s combat readiness significantly. The primary objective of the Dental Services in the field is thus
Ø to provide the dental treatment/oral surgery required by personnel of the DEU and allied armed forces.
Priority must always be given to the preservation or restoration of combat readiness. Repatriation is possible if a dental emergency arises but should always be the option of last resort – for obvious reasons. In almost all cases, personnel and infrastructure provided on location are adequate to the task of dealing with emergencies immediately. On the other hand, definitive surgical revision of wounds and injuries to the soft and hard tissues of the oral region usually requires repatriation, relying on the specialist oral and maxillofacial surgical departments of the DEU AF hospitals, the task for the dental personnel in the field being to provide primary treatment and to enable air transport. Those providing primary treatment in the field require corresponding experience of and skills in oral surgery; for this reason, the dental treatment station in the field hospital in Mazar-e-Sharif is always manned by a dentist/oral surgeon. Allied Personnel stationed at Camp Marmal in Mazar-e-Sharif also make use of the services provided by the dental treatment facilities of the DEU field hospital. For many years, cooperation between the various allied nations represented here has been excellent and essentially unprobematic.
Another important task of the Dental Services is
Ø to provide dental care/oral surgery to members of governmental and non-governmental (GO and NGO) organisations.
There many civilian organisations active in operational regions. Since members of these organisations normally do not have their own medical support, they have to rely on the dental and medical services available locally, including the DEU medical facilities. Although treatment of the local population is not part of the official assignment, such services may be provided by the dental service on humanitarian grounds providing sufficient capacity.
Ø Special assignments
Depending on location and situation, dental personnel may be required to provide services that are not typically with dental care. In Kunduz, for example, dental personnel are involved in obtaining fresh blood donations or assisting in the shock room and operating theatre. Dental expertise may also be required for the identification of victims on the basis of dental protocols.
In view of this complex spectrum of tasks, it is important to ensure that only fully qualified and experienced medical/dental officers are deployed. Medical personnel in the field must be competent to decide on an appropriate course of action without immediate assistance. To make this possible, the DEU AF dental service has established a program of continuing education as well as courses to obtain additional qualifications.
Infrastructure, materials and equipment
To be able to administer adequate oral surgical procedures, dental officers require special devices, instruments and infrastructure. With increasing experience in the field, these fundamentals have been improved and refined significantly.
Although it is possible to provide dental treatment in specially designed dental containers, those available to the DEU AF have not been in use lately, due to several drawbacks. They are kept in store remaining an option for use outside protected bases.
Apart from the seaborne type provided in support of Operation Atalanta, all current dental treatment facilities are located in fortified bases. The largest such facility in the field is part of the field hospital in Mazar-e-Sharif. Let us look at this facility in some detail:
Mazar-e-Sharif Dental Group
At the largest DEU military base in Afghanistan some 3000 German service personnel are stationed. In 2007, the German field hospital was relocated to a newly constructed building complex. The Dental Group is accommodated in the out-patient wing representing the largest section with eight rooms at its disposal. All facilities are generously proportioned and equipped with air-conditioning. There are two treatment rooms,.
The two treatment rooms, each with a state of the art dental chair, are provided with dental instruments and equipment equal to the task of treating patients in the field – including oral surgery. Emergency sets – including those for osteosynthesis and for alveolar bone surgery - are kept at the ready at all times.
The new Dental Group has recently been supplied with a modern digital radiology system that provides for excellent imaging of oral structures while limiting exposure to radiation to a minimum. Monitors in the treatment rooms allow instant imaging and evaluating, while individual prints can be taken simultaneously; for panorama images, there is a designated radiology room.
Accommodation in a fixed, permanent structure increases the safety of the personnel stationed here, particularly if the base is under attack. Since dental section and field hospital are connected, protected passage to and from both parts is available in case of alarm or emergency in the camp. Full air-conditioning allows personnel to remain at their posts for longer periods without experiencing heat-related stress. Considering the fact that external temperatures can be close to 50°C in summer, this is of great benefit to dental personnel and patients alike. Also, there are fewer problems with temperature-sensitive dental materials. This protected environment significantly reduces contamination with the ever-present dust. Finally, the immediate neighbourhood to other medical departments makes interdisciplinary collaboration easier.
On-board dental station
For personnel participating in the sea-borne Operation Atalanta dental care is provided in a dental station on a frigate. Due to the very limited space on board, there is no room exclusively dedicated to dental treatment. The dental station is part of the sick bay; the operating table of the ship’s surgeon can be used as a dental chair.
For more information, please look up an article on dental treatment on sea-going units of the German Navy see published in MCIF 1/4-2011.
Dental diagnoses and treatments in the field
As indicated above, while dental emergencies in the field can be significantly reduced by appropriate prophylactic measures, the cannot totally be eliminated. It is the principal objective of the DEU dental service to further reduce the numbers of such incidents. Therefore, statistics of emergency cases and treatment provided in the field must be of considerable interest. The following section shows a review and analysis of all dental emergency cases documented in 2010 that occurred on land and at sea.
Dental diagnoses
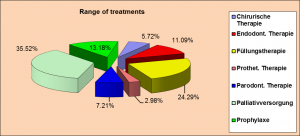 Fig.3: Dental treatments provided in the field. Graphic: SanABw Abt. VI
Fig.3: Dental treatments provided in the field. Graphic: SanABw Abt. VI
A total of 6009 dental treatment sessions were registered in 2010. The ailments were distributed across the spectrum of dental disciplines. In the largest proportion of cases, 27.84%, equivalent to 1673 sessions, conservative dysfunction was diagnosed. This included loss or fracture of fillings and carious defects. Also associated with conservative treatment were the 845 sessions involving endodontic intervention, constituting 14.06% of all sessions. Almost the same proportion of sessions (14.28%, equivalent to 858 sessions) was devoted to treatment of inflammatory processes such as pericoronitis and pulpitis. A relatively large proportion of sessions (10.23% or 615 treatment sessions) involved periodontological disorders. More precise differentiation is required here as the related problems, such as periodontal abscesses and necrotising ulcerative gingivitis, can considerably impair the general status of the patients and thus their combat readiness. Other diagnoses, such as trauma in the oral, jaw or facial region, defective prostheses and cranio-mandibular dysfunction, were encountered in the field far less frequently. However, it must be borne in mind that an emergency case involving trauma, such as a mandibular fracture, has considerable impact on the individual and may make repatriation necessary. It is interesting that the largest proportion of sessions, 29.62%, can be subsumed as “Other”. These sessions are associated with a wide range of different problems (e.g. hypersensitivity of the tooth neck) that cannot be directly related to standard diagnoses. Because of this, it would be advisable to adopt a more differentiated approach to the documentation of cases when developing a future registration system. In addition, emergency cases should, in general, be subjected to a more systematic medical approach. Despite the extensive dental remedial program in the homeland, the number of emergency cases that occurred in the field was not inconsequential. One reason for this may be that we as yet have too little specialist knowledge with regard to various aspects. Insufficient attention has been paid to date to the possible correlations between the stress experienced by personnel on active service and its effects on the aetiology of inflammatory processes. The DEU AF dental service should undertake appropriate research projects in the sector of military dental health in order to obtain more data in this area.
Dental treatments in the field
As shown above, the majority of sessions were devoted to conservative dental problems requiring conservative dental treatment.
(Fig. 3)
Fillings were provided in 1443 sessions, equivalent to 24.29% of all treatment sessions. Another 11.09% of cases involved conservative therapy in the form of endodontic treatments (659 sessions). It is pleasing to note that a relatively high number of treatment sessions (783 or 13.18%) provided in the field were devoted to prophylactic measures. The necessity for these becomes apparent if looking at just at two factors: under the stress of combat conditions soldiers pay less attention to oral hygiene; a compromised immune system due to physical and psychological stress, sometimes associated with heavy smoking can increase the susceptibility to gingival infections. If combined with the 7.21% of sessions (428) involving periodontal treatments, the proportion of treatments involving periodontal measures was 20.39%. Surgical procedures were conducted in only 5.72% of sessions (340), but these cases are significant in sofar as the diagnosis had a serious impact on combat readiness. As in the case of diagnoses, the largest proportion of treatments involved unspecific disorders. Subsumed under “palliative measures” were 35.52% of treatments (2110 sessions) that are not specifically defined. Again, more extensive differentiation will be needed here in future.
Summary
As a part of the medical support services, dental services personnel participate in the various international missions undertaken by the German Armed Forces. The provision of prophylactic and therapeutic measures at the home base designed to restore and preserve combat readiness of service personnel has proven a significant prerequisite for the dental health of personnel deployed on active service abroad. Only personnel with the appropriate oral status – if necessary, after suitable treatment – should be eligible for deployment. However, even with such a preventative program in place, the risk of dental emergencies in the field cannot be ruled out completely. While the majority of cases encountered in the field requires conservative treatment, well trained personnel and adequate infrastructure and materials have to be provided to be able to also master such emergencies. We must try to reduce the numbers of emergency treatments during deployment through appropriate measures at home. This includes further research projects in the sector of military dental health.
Date: 04/25/2018
Source: MCIF 4/2011


