Article: Lieutenant Colonel Dr Michael Lüpke, MC
Stress as a risk factor?
Possible correlations between stress and the pathogenesis and progression of periodontal disease in Bundeswehr personnel in the field
The mechanism that converts psychosocial stress into a potential inflammatory disorder involves complex interactions between nerves and the immune system. It has also been postulated that psychosocial stress may be a risk factor that influences the development and progression of periodontal disease.
Stress in general and active duty-related stress
 Fig. 1: Treatment of a wounded allied comrade in the trauma room.
Fig. 1: Treatment of a wounded allied comrade in the trauma room.
Exposure to unfamiliar forms of stress that may also be experienced as threatening can result in many forms of physiological and immunological changes in the body. These changes that actually represent no more than a short-term response to this threat can make the individual ill if the stress situation persists for longer periods (chronic stress) and develop into physical problems. Of particular relevance in this context are the inflammatory processes that can be the underlying cause of disorders such as atherosclerosis, inflammatory gastrointestinal conditions, allergies, asthma and a range of neurodegenerative diseases, including multiple sclerosis.
In a series of publications, possible correlations between exposure to stress and the severity of the periodontal problem have been demonstrated. While it is undisputed that microbial plaque should be seen as the main cause of inflammatory periodontal disease, greater attention is being paid to other possible causative factors. Although it is now generally accepted that stress is a predisposing factor for necrotising ulcerative gingivitis, there is still insufficient evidence for a similar connection between psychosocial stress and chronic periodontal disease. There are various possible mechanisms through which the effects of psychosocial stress could influence the development and progression of periodontal disease. Psychosocial stress can impact on physiological and immunological parameters and result in disease-relevant behavioural changes in the affected individual. These alterations to parameters and behaviour may result in modification of the individual’s immune responses. It would appear the cytokine interleukin 1β and the stress hormone cortisol may play a particularly important role here.
The increase in stress levels is a general problem facing society as a whole. Service personnel on active service may represent a particularly high risk group in this context. They are often deployed in the field for longer periods during which they are exposed to a wide variety of generalised and personal stress situations that in many cases exert significant psychological strain on those involved and in extreme cases this can result in the development of major problems, such as post-traumatic stress disorder (PTSD). A recent study undertaken by the German Bundeswehr has confirmed this to be the case. In addition, personnel in the field are often also exposed to physical stress factors, such as lack of sleep and extreme climatic conditions.
The question of whether and to what extent active duty-related stress can promote the development and/or progression of inflammatory periodontal disorders is thus a matter that must be of significant interest to military medicine.
The term ‘stress’ is fairly loosely used in common speech and its actual meaning should thus first be considered. ‘Stress’ is derived from the Latin stringere (= to draw tight) and is defined as “a state of tension in which the individual feels that a situation conceived as very unpleasant that will occur in the near future or that has already been subjectively experienced for a longer period is no longer fully under their control although, at the same time, it is subjectively important to that individual to avoid that situation” (from: Aichinger, C., 2003. Arbeitszeit und Subjektive Gesundheitsaspekte, Linz). It should be borne in mind, however, that not all challenges to which an individual is exposed necessarily cause that individual to experience stress. Only when certain circumstances are in place is it absolutely correct to speak of stress. For example, there must be a negative imbalance in the way that the challenge is subjectively perceived and the way that the resources available to counter that challenge are seen. There can be extensive variations in the way that individuals subjectively perceive and evaluate these factors. One and the same stimulus may have a completely different subjective effect in different individuals. Another requirement is that the imbalance between challenge and available resources must be perceived by the individual in question as a genuine threat. This will result in a feeling of inadequacy, to which the body will react with psychological symptoms (e. g. anxiety) and physical symptoms, involving a series of changes to physiological parameters (e. g. in the hormone system, see below for a more detailed discussion). However, in a healthy stress situation, the perceived imbalance between resources and challenge may be something that the individual is willing to overcome, and in this case there is no feeling of inadequacy and thus little or no accompanying psychological or physical symptoms. It is difficult to diagnose stress precisely and accurately; stress-related disorders often only become manifest as a consequence of their physical and psychological effects. Serious psychological disorders, such as depression, can develop as a result of chronic exposure to stress. There are many studies that have demonstrated a significant increase in the incidence of disorders of this kind in recent years in Germany.
Bundeswehr personnel on active service live in Afghanistan, the country of deployment, in camps determined by their operational area and mission and under conditions that are difficult and often extreme, meaning that they are exposed to significantly increased levels of psychological and physical stress. The various stress factors to which they are exposed can be roughly classified as general and individual stress factors. General stress factors may take the form of lack of sleep, thirst and exposure to the extremely high temperatures that in summer can reach 50°C. Individual stress factors can be homesickness, worries about partners at home, loss of comrades and the threat to own life and limb. It is important to bear in mind that the first three stress factors may also impact on service personnel who remain in the supposedly ‘safe’ camp area and are not required to leave it (Fig. 1). Those who, like the author, have been present during vigils for fallen comrades will know that distress is not held at bay by the walls of a camp and can cause appropriate stress reactions. At the same time, those who are required to go on patrols or missions outside the camp are, of course, subject to particularly high levels of stress because of the risk of being killed or wounded.
The Institute of Clinical Psychology and the Centre of Clinical Epidemiology and Longitudinal Studies (CELOS) of Dresden University of Technology are currently undertaking a major study of the psychological effects on Bundeswehr personnel of deployment abroad. The initial results have already been published (there is insufficient space in this article to discuss these in any detail). These show that there is a 6 - 10 times higher risk that personnel who have completed a mission with the ISAF will develop post-traumatic stress disorder (PTSD). The authors[cl1] also point out that it is unwise to concentrate on PTSD alone and ignore other related conditions. They cite in particular anxiety, depression and somatoform disorders that can often remain undiagnosed and thus untreated, and so can significantly exacerbate if the individual remains exposed to deployment-related stress. Such potential traumatic effects of stress must thus also be taken into account.
There are various possible pathomechanisms through which the effects of stress can promote the development of periodontal disease. Before looking at these in more detail, it will be helpful to consider the aetiology of chronic inflammatory periodontal disease.
Aetiology of gingivitis and periodontitis
 Fig. 2: Supragingival microbial plaque – staining has been used to enhance appearance.
Fig. 2: Supragingival microbial plaque – staining has been used to enhance appearance.
According to our current understanding of the mechanism, intraoral bacteria in the supra- and subgingival plaque play a significant role in the development of gingivitis and periodontitis (Fig. 2). These microorganisms have special adhesive properties that allow them to attach themselves to the surface of teeth, where they form complex supra- and subgingival biofilms. A ‘biofilm’ is an organised aggregation of microorganisms on a solid surface. The bacterial configuration of a biofilm is not just random, but exhibits specific spatial and functional arrangements. The formation of a biofilm commences, assuming that plaque is allowed to accumulate without hindrance, with the attachment of primary colonisers that tend predominantly to be facultatively anaerobic Gram-positive cocci (such as Peptostreptococcus micros). According to more recent findings, different microorganisms may be involved in the initial stages of biofilm formation depending on its location. While Streptococcus spp. dominates in the early phases of biofilm formation in supragingival locations, this role is assumed by Lactobacillus spp. in the subgingival region. Some 2 - 3 days later, secondary colonisers join in; these are usually Gram-negative bacteria (such as Aggregatibacter actinomycetemcomitans and Prevotella intermedia). After approximately 7 days, the presence of fibrils [spirilla?] [cl2]and spirochetes can be detected. As the thickness of the biofilm increases, the proportion of Gram-negative microorganisms in it also grows, representing an additional problem for the host. The biofilm forms a protective shield against responses on the part of the host, such as attacks by the host’s antibodies and local antimicrobial treatment with antibacterial mouth washes, for example. The thicker the biofilm becomes, the more diffusion in and out of it is prevented, promoting the development of anaerobic conditions deep inside the plaque. Following appropriate longer exposure to this plaque, chronic gingivitis will develop in its various stages.
 Fig. 3: Clinical signs of necrotising ulcerative gingivitis showing necrosis of the interdental papillae.
Fig. 3: Clinical signs of necrotising ulcerative gingivitis showing necrosis of the interdental papillae.
A chronic gingivitis can remain stable over the long term and there need not be any involvement of other periodontal structures and the onset of periodontitis. In order for periodontitis to develop, it seems that several factors need to be present simultaneously. The pathogens must be in sufficient concentrations in the locality and the host must be appropriately susceptible, both locally and systemically. The local environment must also be suitable to enable the pathogens to develop the required virulence. It is not yet fully understood why periodontitis develops from chronic gingivitis in some cases but does not in others. It is assumed that certain genetic factors, such as interleukin-1 polymorphism, are involved while the influence of other risk factors, such as smoking, on the course of periodontal tissue destruction has been demonstrated.
The necrosis of periodontal tissue is not a continuous process. Periodontitis is episodic, with phases of periodontal destruction followed by inactive phases. Why and how these phases occur is also, as yet, unclear. It is possible that the potency or pathogenic properties of the causative bacterial factor change or that the immune response of the host undergoes modification and that the host thus becomes more susceptible to bacterial attack.
Among the roughly 500 different microorganisms that have been identified in the human oral cavity, certain strains, such as Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis are believed to be facultatively periopathogenic. These are opportunistic microorganisms that are also present in the oral cavity of patients with a healthy periodontium. It would appear that in such individuals, there is an equilibrium between microorganisms and immune response that prevents any infection.
Necrotising ulcerative gingivitis and necrotising ulcerative periodontitis
Necrotising ulcerative gingivitis (NUG) and necrotizing ulcerative periodontitis (NUP) are periodontal disorders that are characterized by rapidly progressive loss of periodontal tissue. When the infection and necrosis remain restricted to the gingival elements of the periodontium, we call this necrotising ulcerative gingivitis. If this remains untreated, the necrosis can spread to other periodontal structures, and develop into necrotising ulcerative periodontitis. The main (and required) clinical signs (Fig. 3) of necrotising ulcerative gingivitis and periodontitis are
- acute and often severe pain
- necrosis and ulceration of the interdental papillae (NUG) and the periodontal ligament and the alveolar bone (NUP)
- spontaneous bleeding
Possible accompanying signs may include
- foetor ex ore
- fever
- significantly compromised general status
- lymphadenitis
- metallic taste in mouth
Service personnel with the above necrotising ulcerative periodontal disorders are not fit for duty; it can be assumed that it will be necessary to take them off the active list if they are present in the field. The causative element will predominantly be a mixed anaerobic microbial flora, containing strains of Treponema and Fusobacterium with Prevotella intermedia and Porphyromonas gingivalis. It has also been postulated that there are a number of possible predisposing factors. It has been demonstrated that psychosocial stress can act as such a predisposing factor. Other possible factors include: HIV infection, immunosuppression, smoking, inadequate oral hygiene, pre-existing gingivitis, relatively young age, malnutrition and undernourishment. It is apparent that service personnel in the field will be exposed to certain of these risk factors. Unfortunately, the German Bundeswehr currently has no credible data on the incidence of NUG and NUP in its personnel on active duty. A detailed survey would provide valuable information.
Stress and the pathogenesis of chronic periodontal disease
So that a stress situation can develop, there must first be an event that is evaluated and assessed by the individual in question. Depending on the result of this evaluation, an emotional response may be triggered and a stress reaction result. As shown in Fig. 1[13], (Fig. 4), the stress reaction can lead to both behavioural changes and modification of physiological parameters.
Stress and behavioural changes
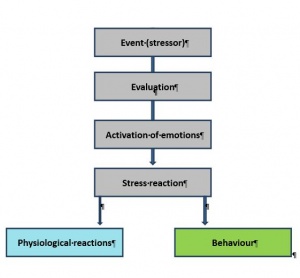 Fig. 4: The development and effects of stress reactions.
Fig. 4: The development and effects of stress reactions.
Stress can result in behavioural changes that are relevant to the development of periodontal disease (Fig. 5). This applies in particular to the oral hygiene of the individual, which is often neglected under chronic stress exposure. This has been shown to be the case in various civilian studies and has been additionally confirmed by studies undertaken by the Bundeswehr. It is interesting to note that the individual concerned is often unaware that they are not paying sufficient regard to oral hygiene, usually because it is not the frequency of their own oral hygiene measures that is reduced, but the efficiency of these measures. The consequence is enhanced accumulation of plaque. This can promote the development of inflammatory periodontal disorders as microbial plaque is the main factor involved in their aetiology. Stress can also influence an individual’s nutritional and eating habits. They tend towards consuming a very one-sided diet, frequently eating carbohydrate-rich foods that, thanks to their high sugar content, also facilitate plaque accumulation. In addition, experts are currently discussing the possibility that there may be an association between nutrition and periodontal health. It is already known that there is a causal connection between vitamin C deficiency and periodontal inflammation – the disease known as scurvy was rife among British sailors in past centuries. But there is as yet no scientific evidence to confirm other possible correlations between nutritional deficiencies and periodontal disease. However, it is at the same time clear that a healthy balanced diet is a requirement for an optimal individual immune status.
Another consequence of exposure to stress can be increased consumption of substances such as alcohol and nicotine. Because of the stringent regulations and lack of availability of high percentage alcohol, it is unlikely that this factor will play a role in the case of personnel in the field. When it comes to smoking, however, the situation is different. The author has no information on whether the Bundeswehr has conducted any surveys of the tobacco consumption of its personnel in the field, but own impressions and observations indicate that personnel on active service smoke unusually heavily. This is almost certainly also attributable to the fact that cigarettes are available where the troops are deployed at a very attractive price as no tax is charged on them. There is a general consensus, supported by the results of numerous studies, that cigarette smoking is a risk factor for the development of periodontal disease and must thus also be interpreted as risk-associated behaviour in this context.
Exposure to stress can also result in reduced utilisation of social networks. Important resources, such as dental care, may be used less frequently or only when it is too late.
Changes to physiological parameters
Stress can also cause pathological changes to physiological parameters. These changes can be extensive and are associated with a wide range of potential reactions. This complexity is due to evolution – we are the descendants of those individuals who survived because they were able to muster all available resources to overcome/rebuff threats to their existence.
The key role in these processes is played by the hypothalamic-pituitary-adrenal axis as this is responsible for converting psychological information into physiological reactions. In response to stress stimuli, the hypothalamus releases corticotrophin-releasing factor (CRF) and arginine vasopressin, which in turn triggers the secretion of adrenocorticotropin hormone (ACTH) from the pituitary gland. ACTH stimulates the adrenal cortex, which releases the glucocorticoids cortisol and corticosterone. It is known that cortisol is an important stress hormone; it mediates a wide range of physiological reactions and has an immunosuppressive potential. It modifies the body’s metabolism and induces the neosynthesis of glucose from protein. From the point of view of possible effects on the periodontium, it may be relevant that cortisol inhibits fibroblast activity, resulting in a loss of collagen and connective tissue. Cortisol activates osteoclasts and may thus also increase the loss of alveolar bone in the periodontium. It also influences the haematopoietic system, suppressing the immune response of the body through lymphocytopenia and thus perhaps upsetting any pre-existing equilibrium between the microbial flora in the gingival and periodontal pockets and the immune response of the host.
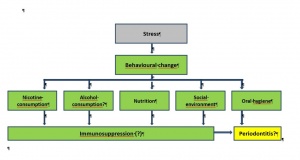 Fig. 5: Potential effects of psychosocial stress on the development of periodontal disease as a result of behavioural changes. Source: Eickholz P, (2005) Ätiologie, 33-70. Bd. Parodontologie 4th edition, Verlag Urban & Fischer, Munich; modified by author.
Fig. 5: Potential effects of psychosocial stress on the development of periodontal disease as a result of behavioural changes. Source: Eickholz P, (2005) Ätiologie, 33-70. Bd. Parodontologie 4th edition, Verlag Urban & Fischer, Munich; modified by author.
When it comes to the possible effects of stress, a particularly significant part could well be played by proinflammatory cytokines, specifically the cytokine interleukin-1β. Interleukins are peptides and are important elements in the inflammatory cascade. It is postulated that there is a close correlation between elevated concentrations of proinflammatory cytokines in the gingival pocket and periodontal inflammation. Interleukin-1β enhances the breakdown of collagen by inducing the formation of collagenase by the gingival and desmodontal fibroblasts and it also inhibits collagen synthesis. It activates adhesion molecules, which enable polymorphonuclear leukocytes to attach to and pass through the vascular wall. It is the most potent osteoclast-activating factor in the human body. In has been demonstrated in various studies that the concentration of interleukin-1β in gingival pockets is elevated in the presence of periodontitis. It was also found that there was a close correlation between the level of interleukin-1β and the severity of periodontal disease. Interleukin-1β is thus an important factor in the pathogenesis of periodontitis as it both promotes inflammatory reactions and is involved in the breakdown of bone tissue. It is interesting to note in this context that there is increased secretion of interleukin-1β in the presence of stress. Prospective studies conducted using as subjects students of dental medicine who were under exam stress report a correlation between level of stress and intrasulcular concentrations of interleukin-1β. It can thus be assumed that troops under active service-related stress will also have elevated levels of intrasulcular interleukin-1β.
The consequences for therapy
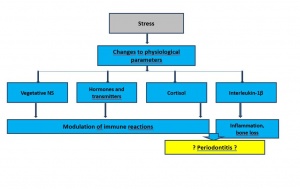 Fig. 6: Potential effects of psychosocial stress on the development of periodontal disease as a result of changes to physiological parameters.
Fig. 6: Potential effects of psychosocial stress on the development of periodontal disease as a result of changes to physiological parameters.
Results of research conducted to date have been unable to find a direct causal connection between psychosocial stress and the development or progression of chronic periodontal disease. However, it can be assumed as a working hypothesis that the mechanisms discussed above are involved in or at least influence the pathogenesis of these disorders. The information available can be used as the basis for the development of helpful therapeutic strategies, particularly when it comes to the stress-induced behavioural changes. Personnel can be informed in advance that they may unconsciously start to neglect their oral hygiene when in the field and be instructed in effective oral hygiene measures. This could be enhanced by additional professional cleaning and scaling shortly after the phases in which personnel are exposed to stress. The Dental Service of the Bundeswehr has already taken a step in this direction by introducing its “Prophylaxis prior to active service” (EVP) programme. It would also appear advisable to provide professional cleaning and scaling services to personnel in the field. However, as there is still no scientific evidence that convincingly shows this to be necessary, it is not currently possible to justify the assignment of additional personnel and infrastructural capacity that would be required to make this reality. At the same time, it must be borne in mind that only troops with a healthy periodontium or who have received the necessary treatment are fit for active service.
The tendency towards reduced use of social networks by those under stress needs to be countered by medical treatment facilities through the use of an appropriate appointment system. It is better to arrange the next appointment with the patient before they leave the dental care facility than to leave the patient to decide in future when they should again report to a dentist.
Date: 11/08/2018
Source: Medical Corps International Forum 2/2013


