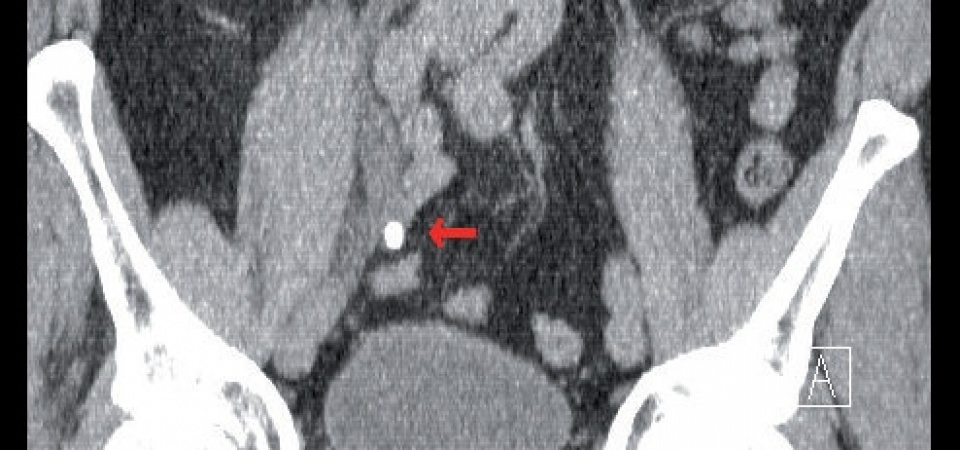
“Low-dose “ CT - coronal images of a
large, right-sided ureteric stone (arrow) with
subsequent proximal urinary retention.
Article: D. REITZEL (GERMANY)
Modern Urological Therapy of Calculi during Deployment
This article discusses stone therapy on deployment. The focus will be on the symptomatic and causal therapy of colic resulting from ureteric stones in order to facilitate the fastest possible restoration of the soldier's fitness for deployment.
The prevalence of urolithiasis in Germany is around 4.7%. The number of new cases has tripled over the 10 years up to 2000 from 0.54 to 1.47%. This condition is now termed a widespread disease and the global trend continues to push upwards.
Introduction
Of course, young, athletic soldiers are not classical stone-formers; however, from the American deployment in Iraq, colic-related admissions to one field hospital, for example, were reported at a rate of 8%. Deployments in hot and arid regions in particular can lead to stone formation if fluid intake is inadequate. This situation is known to cause concentration and therefore over-saturation of the urine with lithogenic substances. The actual amount of fluid required can be reduced by situations of stress, the need to urinate more frequently and other factors. A diet containing high protein and salt levels can also encourage stone formation.
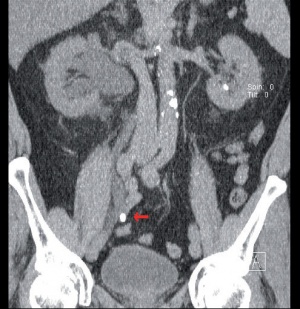 “Low-dose “ CT - coronal images of a
large, right-sided ureteric stone (arrow) with
subsequent proximal urinary retention.
“Low-dose “ CT - coronal images of a
large, right-sided ureteric stone (arrow) with
subsequent proximal urinary retention.
An American study investigated the time to formation of symptomatic stones in deployment conditions among civilian and military personnel in South West Asia and was able to demonstrate that this time was on 93 days on average. This means it is perfectly possible for climatic conditions to lead to stone formation and potential subsequent symptoms of colic among German soldiers as a result of the factors outlined above and the length of deployment. This article primarily discusses stone therapy on deployment and not the treatment of asymptomatic kidney stones. As a result, other treatment methods such as extracorporeal shock wave lithotripsy (ESWL) and percutaneous nephrolitholapaxy (PNL) will not essentially be mentioned any further, since they are of no primary relevance. The focus will be on the symptomatic and causal therapy of colic resulting from ureteric stones in order to facilitate the fastest possible restoration of the soldier's fitness for deployment.
Diagnosis
The diagnosis of ureteric colic essentially comprises a thorough history, clinical examination, laboratory results, ultrasound and, if the suspicion of a stone is high, a native "low-dose" CT scan.
The clinical picture of colic is characterised by often very severe and cramp-like pain, which ceases intermittently but can also be continuous. Depending on the localisation of the stone, the pain typically radiates to the flank, the upper, middle and lower abdomen, or to the groin region with radiation to the scrotum / labia or tip of the penis. Distal or intra-mural stones can lead to increased urgency and pollakiuria. The severity of colic symptoms are not an indicator of the size of the stone, however. Colic patients characteristically have a degree of motor restlessness. Concomitant autonomic reactions include sweating, nausea and vomiting (50% of all colic patients) and possibly a reflectory intestinal paralysis to ileus stage. Laboratory investigations should check the following parameters: urine (urine status / sediment and urine culture (mid-stream urine)) and blood (blood count, creatinine, urea, electrolytes (potassium, calcium, urate), C-reactive protein (CRP) and clotting).
 Image of the same stone in the
transversal view.
Image of the same stone in the
transversal view.
Although microscopic haematuria is very common with colic, its absence does not rule out ureterolithiasis. An increase in retention parameters indicates the extent of renal function impairment as a consequence of urinary retention. Marked leucocytosis and raised CRP with or without leucocyturia indicates an infection, which is complicating the situation. Calcium and in particular uric acid, as well as the urine pH level, can be indicators of the stone composition and therefore provide a guide for further treatment options.
Alongside the clinical examination with classic pain on percussion of the flank, one of the most important, simplest and quickest investigations is an ultrasound of the kidneys. In most cases, a hypo-dense, finger or bud-sized widening of the central reflective bad of the kidney or pelvicocaliceal system is easy to recognise and is an expression of the impairment of urinary drainage. Accessory stones may also be seen in the calices and also in the renal pelvis, as well as at the pyelo-ureteral junction and, if the bladder is full, intramurally. Stones in the ureter itself cannot be seen on ultrasound in adults.
If the picture of clinical symptoms and ultrasound indicates ureterolithiasis, a native, "low-dose" CT scan should be carried out to confirm the diagnosis. This procedure has now completely superseded the plain abdominal X-ray with consecutive contrast medium micturition urogram (MUG). Thanks to its greater sensitivity and specificity with a comparably low dose of radiation, it is superior to the MUG (low-dose CT: 0.97 - 1.9 mSv, MUG 1.3 - 3.5 mSv, conventional plain abdominal film 0.5 - 1 mSv) when not considering a chronological and functional statement regarding the empty system and a direct comparison between X-ray-opaque and X-ray-transparent stones, such as urate stones. Modern "dual-energy" CT scanners already introduced in some military hospitals (not on deployment), however, can also show even these differences in colour.
Treatment of Colic
The concept of administering butylscopamine (Buscopan®) and novamine sulfone, as has been common practice until only recently, is anachronistic and obsolete, since this no longer represents approved guidelines - especially since novamine sulfone is only approved nowadays for this indication when other analgesics have failed.
 X-ray of the right hemi-abdomen with
double-J catheter in situ for a stone in the
medial ureter, with incidental findings of
multiple renal pelvis stones.
X-ray of the right hemi-abdomen with
double-J catheter in situ for a stone in the
medial ureter, with incidental findings of
multiple renal pelvis stones.
Guideline-appropriate therapy involves the administration of non-steroidal anti-phlogistics (NSAP). Oral medications in colic patients are less suitable due to the potential concomitant nausea and vomiting. In this case, the intravenous administration of 50 mg dexketoprofen (Sympal® injection) or ibuprofen as suppositories is recommended. If analgesia is inadequate, we recommend the administration of piritramide (Dipidolor®). The use of pethidine (Dolantin® is not recommended in the guidelines. Tramadol should also not be used for the treatment of colic so as not to limit an escalation in analgesia with more potent opiates. Excessive hydration should be avoided under all circumstances. Of questionable benefit, it has a negative impact on the patient's pain situation as a result of increased urine production with a consequent increase in pressure in the renal pelvic cavity system and can, in worst-case scenarios, lead to fornix rupture. Only if vomiting is severe should adequate fluid substitution be provided. If treatment with medication fails to resolve the colic, urinary drainage from the kidney is required, for instance through the insertion of a double J catheter. As a result of the distension of the renal pelvic cavity system by the obstructing stone and the urinary retention, a complex pathophysiological mechanism triggers hyper-peristaltic waves in the ureter arising from the renal pelvis. The insertion of a double J catheter not only relieves the cavity system but also stops this peristalsis and results in passive dilatation of the ureter with cessation of the colic pain.
Conservative Stone Therapy, MET ("Medical Expulsive Therapy")
For stones measuring < 1 cm, if there is no indication for immediate stone removal or urinary drainage, a watch-and-wait policy can also be adopted. MET ("medical expulsive therapy") makes passage of the stone easier and episodes of colic can be avoided. Assuming that around 95% of all stones with a diameter of < 4 mm are passed after around 40 days, regardless of their localisation, this may be acceptable if there are no symptoms under non-deployment conditions, however this is not so for soldiers who are sick on deployment. Of importance for the decision to adopt a conservative approach in this context is not only the size of the stone but also of course its location and a continuous, rapid expulsion progress. With small stones in the medial and distal ureter especially, a conservative approach can be considered. The treatment schedule used here primarily involves the prescription of Tamsulosin 1 x 0.4 mg ("off-label use", however in accordance with the Guidelines of the European Association of Urology (EAU) and methylprednisolone 2 x 4 mg. The effect of methylprednisolone (anti-oedematous effect on the urothelium) is however regarded as marginal. Alpha-blockers such as Tamsulosin, and even to a smaller degree calcium channel blockers, not only improve stone passage, but also avoid the recurrence of colic. MET therefore also reduces the need for analgesia. If colic pain occurs
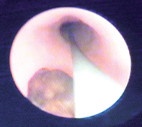 Ureteroscopy: safety wire in situ and
stone.
Ureteroscopy: safety wire in situ and
stone.
again, additional non-steroidal anti-phlogistics (NSAP) can be given as analgesics, such as Diclofenac with gastric cover, or Ibuprofen, bearing in mind retention parameters. Ongoing monitoring can be carried out indirectly with ultrasound (reduction in urinary retention or de-congestion of the kidneys) or with a conventional X-ray (hemi-abdomen). A urine sieve to be used by the patient every time they pass urine can also be helpful for catching the stone. Limiting factors for a conservative approach, even for small stones, include non-resolving colic or patient symptoms, a marked increase in retention parameters with a corresponding urinary retention situation, increased serological infection parameters with or without co-existing urinary tract infection based on urine testing and, of course, the time factor. For stones with a low likelihood of being expelled in particular, interventional treatment should be initiated as soon as possible in order to shorten any treatment interval on deployment. Even with smaller stones, the decision to proceed to an invasive procedure with stone recovery via ureteroscopy or lithotripsy should be made more quickly on deployment; this mainly to restore the soldier's fitness for action, in line with a guidelines-compliant approach - especially since there is a trend observed currently both in non-deployment conditions and in the civilian sector towards rapid (endoscopic) care. The fact that treatment variations are practicable under deployment conditions was illustrated in a publication by Rozanski, in which treatment with double-J catheters performed during the Iraq war ("Operation Iraqi Freedom") as a therapeutic measure was also described without the availability of ureteroscopy equipment alongside the pharmaceutical treatment of urinary calculus colic. In a selected patient cohort (single stone, < 8 mm), thread-armed double-J catheters were inserted which enabled the soldiers to remain in the conflict zone. After 11 - 14 days, the double-J catheter was carefully removed via the threads in the meatus and spontaneous expulsion of the stone was observed within 72 hours.
Interventional Stone Treatment
Interventional treatment options for ureteric stones include extracorporeal shock wave lithotripsy (ESWL) and ureterorenoscopy (URS). Although until recently ESWL was more effective than the more invasive URS for proximal ureteric stones, the age of laser lithotripsies has led to better removal rates for proximal stones > 1 cm, although not for stones < 1 cm. For ureteric stones in the medial and distal third, ureterorenoscopy is the technique of choice.
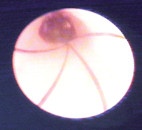 Dormia basket with small stone.
Dormia basket with small stone.
Alongside double-J catheter insertion as a primary temporary solution or as a solution for persistent pain despite adequate analgesia, direct stone removal can also be aimed for. Other indications for double-J catheter insertion include persistent obstruction and urinary retention in patients with solitary kidneys or with pre-existing renal failure, which will tend not to be the case for soldiers on deployment. Experience has shown that the pre-interventional insertion of a double-J catheter for 3-7 days, a procedure known as "pre-stenting", can make stone extraction via ureterorenoscopy easier as a result of the widening of the ureter and ostium caused by the catheter. Depending on the size and position of the stone, however, a URS may primarily be carried out safely and efficiently as an "emergency" URS. The indication for lithotomy for ureteric stones, via open surgery or laparoscopy, remains reserved nowadays to just a few isolated cases where anatomical corrections are also required.
Performing Ureterorenoscopy (URS):
The performance of stone treatment via ureterorenoscopy is carried out on deployment in Mazar-e-Sharif with a semi-rigid ureterorenoscope. Modern semi-rigid ureterorenoscopes today only have an around 6 - 10.5 Charr. external diameter, have fibre-optic illumination and a working and irrigation channel. The optical images are transferred via camera to a monitor. The procedure is usually carried out under general anaesthesia or sometimes also spinal anaesthesia. The guidelines recommend intra-operative antibiotics. The patient is positioned in the lithotomy position. Small stones can be removed directly using a basket. For larger stones, stone shattering (lithotripsy) is required via a lithotripsy probe. Intra-corporeal lithotripsy can essentially be carried out electro-hydraulically, using ultrasound, pneumatic force or with lasers. The "Stonebreaker™" from Cook is used on deployment. This small mobile device generates a shock wave through the stone using a CO2 high-pressure cartridge. The resulting fragments can then be recovered. For very large stones and complex fragment recovery, a "smash-and-go" approach can be taken. The primary goal, however, remains the immediate primary resolution of the stone. Limiting factors for successful ureteroscopy include the visual conditions, which may be considerably impaired as a result of oedematous or inflammatory changes of the ureteric mucosa with subsequent bleeding or also a very prominent stone bed.
Depending on the duration of the procedure or maceration of the mucosa, a double-J catheter can be inserted. This is not absolutely necessary and should not be carried out routinely due to the potential morbidity associated with it. For small stones and uncomplicated URS, no double-J catheter insertion is needed. It is recommended for surgeries lasting more than 45 minutes, bilateral procedures, strictures, proximal stone localisations and for residual stones - including in preparation for a potential secondary procedure - but also in cases of pre-existing renal failure or solitary kidney. It is required where there is heavy mucosa bleeding and if perforation is either suspected or confirmed with the administration of contrast medium.
Double-J catheter symptoms are also expressed in the form of flank pain, bladder pain and cramps, pollakisuria and haematuria. These symptoms can be alleviated by the administration of an alpha blocker.
In the case of an otherwise uncomplicated URS, the double-J catheter can be removed after 3 - 7 days, although following perforation it should remain in situ for at least 4-6 weeks, and possibly longer depending on the lesion. There is no exact data regarding the period for which it must be left in situ and the relevant indications, however. If not all of the fragments of a large stone are removed, MET also improves the expulsion of small residual fragments in this case. An X-ray check (hemi-abdomen) is carried out on the first day post-operatively to exclude potential residual stones. If no interventional double-J catheter was inserted, the appropriate kidney should be scanned with ultrasound at least to exclude any urinary retention.
Contraindications for URS
If there is hydronephrosis with serological signs of infection or a pyrexial urinary tract infection, ureterorenoscopic stone removal is contraindicated, regardless of the size of the stone, and immediate urinary drainage via the trans-urethral insertion of a double-J catheter is required. Alternatively, a renal fistula catheter can be inserted percutaneously under ultrasound guidance. Both procedures are currently regarded as adequate and are available on deployment. The focus lies on decompressing the cavity system in order to resolve infection. Antibiotic therapy can only be effective if the drainage is adequate. Final stone removal only takes place once the infection has been treated; if there is preceding sepsis, then this should only be done following repatriation.
Complications of Ureterorenoscopy
The complication rate of URS is currently stated at 25%. Severe complications such as complete ureteric avulsion occur in fewer than 1% of cases for urologists experienced in endoscopic procedures and must in virtually all cases be treated through open surgery. Ureteric avulsion can occur, for example, after pulling too hard with too large a stone in a stone basket. This typically results in a tear in the proximal part of the ureter or pyelo-ureteral junction. Avulsions in the distal part of the ureter are also possible, however, when ureterorenoscopes with a large external diameter are used and excessive force is used to advance the device. Depending on the localisation, open procedures involving a ureterocystoneostomy are carried out using a "psoas" or "Boari-Hitch"-plasty or, if there is a ureteric avulsion higher up, a renal pelvicoplasty. Because of the ureterorenoscope's potential to strip the ureteric mucosa and increased stricture rates, end-to-end anastomoses are rarely carried out.
Discussion and Conclusions
 Ureterorenoscope (Wolf).
Ureterorenoscope (Wolf).
Should the term "modern" be regarded critically in relation to deployment? Modern stone therapy, especially for ureteric colic, which is relevant to deployment, is characterised by rapid stone release with a simultaneously low rate of morbidity. Semi-rigid ureterorenoscopy with ureterorenoscopes of the latest generation and monitor transfer in combination with an adequately pneumatically, i.e. ballistically, operated lithoptriptor, is perfectly sufficient for deployment and can be regarded as modern. In the hands of an experienced urologist, it is a fast, safe and low-complication option for restoring the soldier's fitness. The question of the practicality of a laser under deployment conditions need to be made dependent on the primary localisation of the stones causing the colic, namely in the ureter. In Europe, flexible ureterorenoscopy with laser lithotripsy is mainly used for stones in the renal pelvic cavity system and is therefore not primarily relevant to deployment, nor are the treatment of kidney stones with ESWL and percutaneous nephrolitholapaxy (PNL).
 "Stonebreaker™" mobile lithotriptor (Cook) with CO2cartridge and lithotripsy probe
"Stonebreaker™" mobile lithotriptor (Cook) with CO2cartridge and lithotripsy probe
All of the modern treatment options for urolithiasis, from flexible ureterorenoscopy and laser lithotripsy to PNL with very small shaft diameters of the PNL sets (mini-PNL), can be maintained within the Bundeswehr's urological capabilities. It is also possible to use extracorporeal shock wave lithotripsy to treat stones with modern lithotriptors, supported by ultrasound or radiological stone localisation and subsequent virtual stone elimination. Consequently, the modern intervention options are supported by excellent treatment and care options of the very highest standard are available in the home country for definitive stone treatment, in cases where stones are too large, for example.
Author:
Lt. Colonel MC Dirk Reitzel
Department of Urology
German Armed Forces Hospital Berlin
Date: 07/15/2019
Source: Medical Corps International Forum (4/2015)


