Report: Reinke
Barodontalgia - Toothache triggered by hypobaric and hyperbaric conditions
Hypobaric and hyperbaric changes can trigger extreme states of pain in the human body. This article focuses on the phenomenon of barodontalgia, describing its pathophysiology and providing suggestions for preventative measures and approaches to treatment based on patient cases.
Introduction
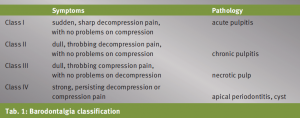 Barodontalgia classification
Barodontalgia classification
Barodontalgia is described as acute toothache with high to extremely high sensitivity, which occurs due to a sudden change in environmental pressure. Therefore not only pilots, divers and skydivers may be affected, but also high-altitude mountain climbers, flight cabin crew and staff that work in medical pressure chambers. Broadly speaking the main condition for barodontalgia is the change in environmental pressure. Remarkably barodontalgia is always triggered by some pathological cause. All literature on this subject describes cases in which one or several causes could have been associated. Here the main triggers identified are inadequate restorations, secondary caries, inadequate root canal fillings, post-operative lesions, or apical or periodontal damage (diagram 1). Information in the literature clearly deviates regarding heights and depths at which barodontalgia may occur (600-12,000 metres/10-40 metres). On average it can be said that barodontalgia occurs at heights of 600 to 1,500 metres and depths of 10 to 25 metres; there is no significant difference of incidence between aviators and divers. At great heights the phenomenon is evident in aircraft with pressurized and non-pressurized cabins, where pain develops more frequently during ascent. For divers pain occurs mostly during descent. Deviations in the literature possibly arise due to retrospective diagnosis, as many studies attribute their results purely to patient information. Patients affected cannot always fully comprehend the circumstances of the incidences when they occur, even understating or overstating them retrospectively.
Background
There is a historical background for the clinical relevance of barodontalgia for military dentists and soldiers. Initially, painful conditions caused by fluctuations in pressure were called aerodontalgia or aerodontopathy, and this phenomenon was first observed with pilots and skydivers during the first and second world wars. Soon after documentation followed regarding divers, high-altitude mountain climbers and medical staff working in pressure chambers. For this reason a uniform nomenclature was required. The term recognised today is barodontalgia.
Dilemma of Diagnosis
 Fig. 1–3: Patient 1
Fig. 1–3: Patient 1
Diagnosis is complicated as it is mostly multifactorial and heavily dependent on patient information, as it is not possible to imitate and recreate the conditions triggering the complaints under dental practice conditions. The better the patient can explain their condition, the more likely a diagnosis can be made. Examinations often highlight multiple lesions where the differential diagnosis does not always provide precise indications regarding the genesis of the respective case. Whether barodontalgia would disappear after treatment of the evident dental insufficiency can only really be examined if the same or similar pressure conditions were prevalent and the pains did not reoccur. It is presumed that without therapy the pains would return with the same intensity. It is clear from the aforementioned definition that the conditions of barodontalgia can be prevented. For this purpose, however, the awareness of the trigger factors and the pathology of barodontalgia is important, so that all patients can be individually advised and cared for. The study design of most research undertaken on this subject highlights several professional groups, (pilots, divers, skydivers), who are particularly predestined to develop barodontalgia. In addition to these specialists, however, any soldier to be deployed abroad should have an entry examination of the predilection sites mentioned. Aeroplanes are usually used to move troops due to the displacement of operational areas, and thus all soldiers are potential risk patients during transportation. The subject of barodontalgia is pertinent to military medicine as often very sensitive, dangerous and strategic duties are undertaken by vulnerable persons, and an acute and intense pain can quickly become a life-threatening situation. On the one hand for the person concerned, but also for those soldiers depending on him. A soldier of this patient group has to undertake important orders during operations, he cannot be absent for a long period of time and usually cannot be replaced on an ad hoc basis. In addition, the orders of other units often tactically depend on specialised personnel. Furthermore, the exacerbation of different dental complaints occurring under high stress levels, lacking hygienic conditions and exposure to germs is often more potent in the deployed country than at home.
Classification
Today the FREJENTSIK and ANKER barodontalgia classification is used most frequently; this divides the condition into four classes. This classification appears to be popular, as it not only explains the symptoms, but also provides information on diagnosis and therapy. As this classification was published in 1983 and dental conservation techniques have developed enormously since then, often individual, adapted therapy solutions can be developed today. An earlier publication by STROHAVER describes a direct (dental genesis) and an indirect type of barodontalgia (barosinusitis, barotitis and bruxism) and combines the symptoms, aetiology, clinical and radiological examination results as well as additional anamnestic aspects.
In the case of barosinusitis a secretion occlusion is usually blocking the natural ostium. When changes in pressure occur the sinus can no longer process the equalisation of pressure. In the case of anatomical variations, such as septum deviations, occlusions are even more frequent. Barosinusitis complaints occur as compression pain and mostly persist after appearance. Pains are often triggered when bowing the head.
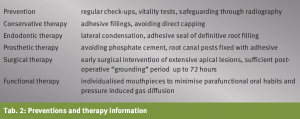 Preventions and therapy information
Preventions and therapy information
The Valsalva manoeuvre can relieve this by causing an active equalisation of pressure. It has often been controversially discussed that bruxism is perhaps a co-factor in the development of barodontalgia states. A study of the Israeli air force showed a high incidence (69%) among young cadet officers in flight duty in comparison to other cadet officers with merely 27%. A progression is also evident among divers and skydivers, most probably due to their essential use of mouthpieces and breathing apparatus. To ensure the permanent seal of the mouthpiece it is necessary to have strong muscle tone. In addition, strong mastication forces are transferred to the mouthpiece due to stressful situations. Jaw complaints or muscular based functional disorders can also be triggered in this way.
Pathophysiology
 Fig. 4–5: Patient 2
Fig. 4–5: Patient 2
The physical basis for barodontalgia is essentially based on Boyle’s law (Boyle-Mariotte law)* and Gay-Lussac’s law**. From a physiological point of view, the compression or expansion of enclosed air bubbles irritates the nerve endings and nociceptors. This ultimately leads to painful sensations, oedemas or even gas embolisms. This genesis of air bubbles and air pockets can be explained through different hypotheses. The first theory implies that inflammation leads to pockets of gas. This could be through infected necrosis or apical abscesses for example, which cause gases due to bacteria. In addition, small defects like carious, undermining dentin lesions with minimal enamel damage, or inadequate edge coverage with caries development, cause air to move between the cavities or even to become trapped inside due to changes in pressure. A second hypothesis is that iatrogenic gas pockets bind together. This can occur through inadequate endodontic condensation, for example. Furthermore air can remain in the operated cavity after surgical procedures, which is only reabsorbed after some time. Gas pockets can also be caused by diffusion. The pressurised air inhaled by divers, jet pilots and extreme skydivers can be so significant that it can easily access inadequate restorations or carious lesions. Above all, the air can also diffuse into the surrounding tissues and lead to strong emphysema type pains. In this context Helium mixtures have been identified to be particularly aggressive. The fourth theory is gas pockets in cavities. In this case the teeth are not affected per se, but the surrounding structures. In patients suffering from sinusitis, a blocked natural ostium can affect the process of pressure equalisation, causing significant projected face pains. This also applies to the ear. In such cases barosinusitis or barotitis media is presented as a differential diagnosis for barodontalgia.
Patient cases
Patient case 1
A Belgian, female, education officer presented symptoms after a flight in a transport aircraft. Some minutes after start-up she experienced a right-sided oppressive, ongoing pain that persisted until landing. The patient still had pain on landing, however, it was alleviated through pressure equalisation techniques (Valsalva manoeuvre). The assessment of results showed several problems.
Radiological imaging of tooth 17 showed a carious defect and the tooth was slightly sensitive to percussion during the negative sensitivity test. Tooth 14 showed an inadequate restoration. In addition, tooth 47 was carious with positive vitality. The root canal filling on tooth 45 was inserted two years ago and here imaging showed an apical osteolysis. Furthermore, there was evidence of a cystic change in the right sinus maxillaris. This case clearly illustrates the problem of diagnosis, as all of the above teeth could have been considered as trigger factors for barodontalgia, yet in the assessment of results all but tooth 17 were symptom free. Tooth 45 was excluded as the sole cause, as the complaint started on ascent. This is typically not the case for an indication of an apical cause. In the same light, tooth 14 was also rather unlikely to be the trigger. Here despite there being a root canal filling, there was evidence of an inadequate post-endodontic restoration. A stimulation of the nociceptors would only be possible here if there was a simultaneously occurring apical osteolysis. Finally, tooth 47 could also be responsible for the onset. However, this could not be the case as the pain also persisted during the compression phase of the flight. The x-ray results and the reduction of the intensity of pain through active pressure equalisation during the flight suggest barosinusitis as the diagnosis. Some authors are of the opinion that barosinusitis is more likely a diagnosis in the majority of unclear cases. However, as the pain had already began on the ascent of the transport aircraft, in this case the origin was a combination of dental causes, based on tooth 17, and projected pain based on cystic changes in the sinus.
Patient case 2
A German paratrooper presented symptoms on returning from holiday. He tried diving again after two years of abstinence and experienced significant pain whilst diving. The pain quickly disappeared after the dive, however, the next day the severe pain returned. The several hour return flight, however, proceeded without problems.
According to the patient, tooth 36 was endodontically treated half a year ago and reacted slightly to percussion. The x-ray showed a larger cavity between the filling and pulp floor. After removal of the filling a tear was evident on the pulp body, an extension of the previously detected buccal tear. The tooth however was not completely fractured. Detailed examination of the x-ray image showed a bifurcation fracture. Understanding the genesis of the problem that occurred was difficult, as no comparable patient documents existed. It could not be understood whether partial odontocrexis was triggered by an increase in pressure, or was purely caused by the under-served, destabilised, post-endodontic situation. The results of the studies by CALDER and RAMSEY, which focus on the frequency of odontocrexis, suggest that the tear in the hard substance was pressure-induced. They showed that in particular inadequately restored teeth, are likely to fracture under pressure, whereby it is mainly the tooth substance that fractures, rarely the restoration. Conversely a French article describes the instance of odontocrexis on the native tooth of a pilot and therefore challenges the theory that pressure-induced fractures only affect inadequately restored teeth.
Patient case 3
A US American infantry soldier showed a slight swelling in the area of the left canine fossa. He reported intermittent problems when chewing which could be reduced with analgesics. Due to his regular search and clear operations outside of the forward operation base, as well as a lack of sleep and emotional stress, he himself was aware of his poor oral hygiene.
The pain started suddenly during a half hour flight and also persisted after landing. Generalised gingivitis was in fact established. In addition, the patient was treated with a partial prosthesis in the lower jaw. Clinically inadequate fillings of teeth 21 and 22 were apparent; 22 was extremely sensitive to percussion with negative vitality. The x-ray showed an apical explanation. The diagnosis was unquestionable based on the symptoms of barodontalgia class IV, in the sense of FREJENTSIK and ANKER's classification. However, the patient’s case demonstrated the importance of fully assessing patient’s results before deployment abroad. The patient was in Afghanistan only eight weeks. It must therefore be assumed that the bone lesion had already been diagnosed prior to deployment in the detailed assessment, according to STANAG 2466. However, according to the patient information there was no radiological assessment of results and no vitality test was undertaken.
Prevention and Therapy
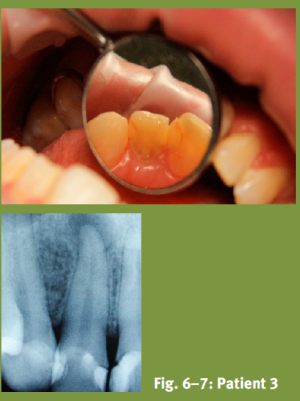 Fig. 6–7: Patient 3
Fig. 6–7: Patient 3
It is evident from the case examples and the definition of direct barodontalgia conditions that adequate prophylactic measures can significantly reduce the incidence. Furthermore, effective and complete assessments for predestined staff must be more thoroughly examined. Here the focus lies on soldiers who are constantly exposed to pressure, but non-flight staff should also be examined in detail before deployment abroad. Aircraft is the most used method of transport for relocation during deployment, for changing location during operation and also for medical evacuation scenarios. During maritime operations dives occur worldwide, and therefore specialised screening of maritime divers would also be beneficial. Table 2 shows an overview of the generally recognised recommended therapy. The majority of studies on the subject of barodontalgia are retrospective or based on in-vitro tests. The problem to-date has been the transferability of data collected during experiments to the clinical situation. Nevertheless, the subject arouses more and more scientific interest. An earlier examination for example showed that teeth with an adhesive restoration were pressure-stable up to 5.0 bar and therefore fractures could be minimised. Dive experiments have also shown that the use of temporary medical inserts can enable pressure equalisation and consequently pressure exposure does not have to be prevented during this phase of endodontic therapy. In comparison to this however, exposure should be avoided after a permanent root canal filling without final adhesive restoration. Furthermore, several studies show the importance of condensation techniques for root canal fillings. Here it seems that for persons under pressure the careful application of a warm filling technique is advantageous.
To avoid the early detachment of prosthetic restorations, no cement should be used for fixation. MUSAJO et al. and LYONS et al. support the opinion that between the cement particles enclosed air can lead to microporosity in the structure during pressure fluctuations and thus reduce retention force. This loss of retention force could also be demonstrated by simulated dives with post-endodontic inserted root canal pins.
In reference to surgical measures for persons under pressure, some authors support the opinion that a premature resection of the apex of the dental root, or prophylactic removal of the wisdom teeth could prevent barodontalgia. In instances were surgical measures have taken place, at least 72 hours must have elapsed before the patient is exposed to pressure.
To avoid parafunctional habits, prosthetic work for the placement of breathing apparatus must be closely examined. A Dutch study generally recommends that individualised mouthpieces are produced for patients with increased risk. Cost would clearly not be a negligible factor here, however, at least patients with partial prostheses should contemplate this solution.
Summary
Hypobaric and hyperbaric conditions, and primarily their rapid variations, can lead to acute pain in the human body. Barodontalgia therefore represents a diagnostic challenge. Knowledge on this subject of dental medicine is urgently required by military dentists when dealing with predisposed patients. Particularly mentioned are divers, pilots and sky divers, but any soldier could also become a risk patient. This article merely provides an introduction to this subject area. It should however raise awareness, as new research shows that there are promising findings in basically all areas – from preventative measures to surgical therapy approaches. If these recommendations are observed in the future, they could assist in the reduction of incidence. Furthermore, therapy procedures undertaken by clinicians must be effectively planned and individually adapted to specialised personnel. In addition, regular check-ups are absolutely necessary.
Date: 02/21/2019
Source: Medical Corps International Forum (1/2014)